Chikungunya
| Chikungunya | |
|---|---|
 | |
| Rash from chikungunya | |
| Pronunciation |
|
| Specialty | Infectious disease |
| Symptoms | Fever, joint pain[2] |
| Complications | Long term joint pain[2] |
| Usual onset | 2 to 12 days after exposure[3] |
| Duration | Usually less than a week[2] |
| Causes | Chikungunya virus (CHIKV) spread by mosquitoes[3] |
| Diagnostic method | Blood test for viral RNA or antibodies[3] |
| Differential diagnosis | Dengue fever, Zika fever[3] |
| Prevention | Mosquito control, avoidance of bites[4] |
| Treatment | Supportive care[3] |
| Prognosis | Risk of death ~ 1 in 1,000[4] |
| Frequency | > 1 million (2014)[3] |
Chikungunya is an infection caused by the Chikungunya virus (CHIKV).[3] Symptoms include fever and joint pains.[2] These typically occur two to twelve days after exposure.[3] Other symptoms may include headache, muscle pain, joint swelling, and a rash.[2] Symptoms usually improve within a week; however, occasionally the joint pain may last for months or years.[2][5] The risk of death is around 1 in 1,000.[4] The very young, old, and those with other health problems are at risk of more severe disease.[2]
The virus is spread between people by two types of mosquitos: Aedes albopictus and Aedes aegypti.[3] They mainly bite during the day.[6] The virus may circulate within a number of animals including birds and rodents.[3] Diagnosis is by either testing the blood for the virus's RNA or antibodies to the virus.[3] The symptoms can be mistaken for those of dengue fever and Zika fever.[3] After a single infection it is believed most people become immune.[2]
The best means of prevention is overall mosquito control and the avoidance of bites in areas where the disease is common.[4] This may be partly achieved by decreasing mosquitoes' access to water and with the use of insect repellent and mosquito nets.[3] There is no vaccine and no specific treatment as of 2016.[3] Recommendations include rest, fluids, and medications to help with fever and joint pain.[3][2]
While the disease typically occurs in Africa and Asia, outbreaks have been reported in Europe and the Americas since the 2000s.[3] In 2014 more than a million suspected cases occurred.[3] In 2014 it was occurring in Florida in the continental United States but as of 2016 there were no further locally acquired cases.[7][8] The disease was first identified in 1952 in Tanzania.[3] The term is from the Kimakonde language and means "to become contorted".[3]
Signs and symptoms
The incubation period ranges from one to twelve days, and is most typically three to seven.[9] The disease may be asymptomatic, but generally is not, as 72% to 97% of those infected will develop symptoms.[9] Characteristic symptoms include sudden onset with high fever, joint pain, and rash. Other symptoms may occur, including headache, fatigue, digestive complaints, and conjunctivitis.[10]
Information gained during recent epidemics suggests that chikungunya fever may result in a chronic phase as well as the phase of acute illness.[11] Within the acute phase, two stages have been identified: a viral stage during the first five to seven days, during which viremia occurs,[12] followed by a convalescent stage lasting approximately ten days, during which symptoms improve and the virus cannot be detected in the blood.[9] Typically, the disease begins with a sudden high fever that lasts from a few days to a week, and sometimes up to ten days. The fever is usually above 39 °C (102 °F) and sometimes reaching 40 °C (104 °F) and may be biphasic—lasting several days, breaking, and then returning. Fever occurs with the onset of viremia, and the level of virus in the blood correlates with the intensity of symptoms in the acute phase.[12] When IgM, an antibody that is a response to the initial exposure to an antigen, appears in the blood, viremia begins to diminish. However, headache, insomnia and an extreme degree of exhaustion remain, usually about five to seven days.[13]
 Chikungunya abdomen
Chikungunya abdomen Chikungunya (lower extremeties)
Chikungunya (lower extremeties) Symmetrical inflammatory polyarthritis of the small joints of the hands and tenosynovitis of the wrist joints in a patient with chronic stage of Chikungunya fever
Symmetrical inflammatory polyarthritis of the small joints of the hands and tenosynovitis of the wrist joints in a patient with chronic stage of Chikungunya fever
Following the fever, strong joint pain or stiffness occurs; it usually lasts weeks or months, but may last for years. The joint pain can be debilitating, often resulting in near immobility of the affected joints.[14] Joint pain is reported in 87–98% of cases, and nearly always occurs in more than one joint, though joint swelling is uncommon.[9] Typically the affected joints are located in both arms and legs, and are affected symmetrically. Joints are more likely to be affected if they have previously been damaged by disorders such as arthritis.[11] Pain most commonly occurs in peripheral joints, such as the wrists, ankles, and joints of the hands and feet as well as some of the larger joints, typically the shoulders, elbows and knees.[9][11] Pain may also occur in the muscles.[15]
Rash occurs in 40–50% of cases, generally as a maculopapular rash occurring two to five days after onset of symptoms.[9] Digestive symptoms, including abdominal pain, nausea, vomiting or diarrhea, may also occur.[9][10][16] In more than half of cases, normal activity is limited by significant fatigue and pain.[9] Infrequently, inflammation of the eyes may occur in the form of iridocyclitis, or uveitis, and retinal lesions may occur.[17]Temporary damage to the liver may occur.[18]
Rarely, neurological disorders have been reported in association with Chikungunya virus, including Guillain–Barré syndrome, palsies, meningoencephalitis, flaccid paralysis and neuropathy.[10] In contrast to dengue fever, Chikungunya fever very rarely causes hemorrhagic complications. Symptoms of bleeding should lead to consideration of alternative diagnoses or co-infection with dengue fever or coexisting congestive hepatopathy.[12]
Chronic disease
Observations during recent epidemics have suggested chikungunya may cause long-term symptoms following acute infection.[19][20][21] This condition has been termed chronic Chikungunya virus-induced arthralgia.[4] Long-term symptoms are not an entirely new observation; long-term arthritis was observed following an outbreak in 1979.[22] Common predictors of prolonged symptoms are advanced age and prior rheumatological disease.[23][24][25][26]
During the La Reunion outbreak in 2006, more than 50% of subjects over the age of 45 reported long-term musculoskeletal pain[24] with up to 60% of people reporting prolonged painful joints three years following initial infection.[23] A study of imported cases in France reported that 59% of people still suffered from arthralgia two years after acute infection.[27] Following a local epidemic of chikungunya in Italy, 66% of people reported muscle pains, joint pains, or asthenia at one year after acute infection.[25]
Currently, the cause of these chronic symptoms is not fully known. Markers of autoimmune or rheumatoid disease have not been found in people reporting chronic symptoms.[23][28] However, some evidence from humans and animal models suggests chikungunya may be able to establish chronic infections within the host. Viral antigen was detected in a muscle biopsy of a person suffering a recurrent episode of disease three months after initial onset.[29] Additionally, viral antigen and viral RNA were found in macrophages in the synovial joint of a person experiencing a relapse of musculoskeletal disease 18 months after initial infection.[30] Several animal models have also suggested Chikungunya virus may establish persistent infections. In a mouse model, viral RNA was detected specifically in joint-associated tissue for at least 16 weeks after inoculation, and was associated with chronic synovitis.[31] Similarly, another study reported detection of a viral reporter gene in joint tissue of mice for weeks after inoculation.[32] In a nonhuman primate model, Chikungunya virus was found to persist in the spleen for at least six weeks.[33]
Cause
Virology
| Chikungunya virus | |
|---|---|
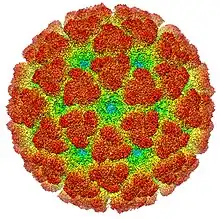 | |
| Cryoelectron microscopy reconstruction of Chikungunya virus. From EMDB entry EMD-5577[34] | |
| Virus classification | |
| (unranked): | Virus |
| Realm: | Riboviria |
| Kingdom: | Orthornavirae |
| Phylum: | Kitrinoviricota |
| Class: | Alsuviricetes |
| Order: | Martellivirales |
| Family: | Togaviridae |
| Genus: | Alphavirus |
| Species: | Chikungunya virus |
Chikungunya virus (CHIKV), is a member of the genus Alphavirus, and family Togaviridae. It was first isolated in 1953 in Tanzania and is an RNA virus with a positive-sense single-stranded genome of about 11.6kb.[35] It is a member of the Semliki Forest virus complex and is closely related to Ross River virus, O'nyong'nyong virus, and Semliki Forest virus.[36] Because it is transmitted by arthropods, namely mosquitoes, it can also be referred to as an arbovirus (arthropod-borne virus). In the United States, it is classified as a category B priority pathogen,[37] and work requires biosafety level III precautions.[38]
Transmission

Chikungunya is generally transmitted from mosquitoes to humans. Less common modes of transmission include vertical transmission, which is transmission from mother to child during pregnancy or at birth. Transmission via infected blood products and through organ donation is also theoretically possible during times of outbreak, though no cases have yet been documented.[11]
Chikungunya is related to mosquitoes, their environments, and human behavior. The adaptation of mosquitoes to the changing climate of North Africa around 5,000 years ago made them seek out environments where humans stored water. Human habitation and the mosquitoes’ environments were then very closely connected. During periods of epidemics humans are the reservoir of the virus. Because high amounts of virus are present in the blood in the beginning of acute infection, the virus can be spread from a viremic human to a mosquito, and back to a human.[39] During other times, monkeys, birds and other vertebrates have served as reservoirs.[40] Three genotypes of this virus have been described, each with a distinct genotype and antigenic character: West African, East/Central/South African, and Asian genotypes.[41] The Asian lineage originated in 1952 and has subsequently split into two lineages – India (Indian Ocean Lineage) and South East Asian clades. This virus was first reported in the Americas in 2014. Phylogenetic investigations have shown that there are two strains in Brazil – the Asian and East/Central/South African types – and that the Asian strain arrived in the Caribbean (most likely from Oceania) in about March 2013.[42] The rate of molecular evolution was estimated to have a mean rate of 5 × 10−4 substitutions per site per year (95% higher probability density 2.9–7.9 × 10−4) typical of RNA viruses.[43]
Chikungunya is spread through bites from Aedes mosquitoes, and the species A. aegypti was identified as the most common vector, though the virus has recently been associated with many other species, including A. albopictus.[11] Research by the Pasteur Institute in Paris has suggested Chikungunya virus strains in the 2005-2006 Reunion Island outbreak incurred a mutation that facilitated transmission by the Asian tiger mosquito (A. albopictus).[44] Other species potentially able to transmit Chikungunya virus include Ae. furcifer-taylori, Ae. africanus, and Ae. luteocephalus.[11]
Mechanism
Chikungunya virus is passed to humans when a bite from an infected mosquito breaks the skin and introduces the virus into the body. The pathogenesis of chikungunya infection in humans is still poorly understood, despite recent outbreaks. It appears that in vitro, Chikungunya virus is able to replicate in human epithelial and endothelial cells, primary fibroblasts, and monocyte-derived macrophages. Viral replication is highly cytopathic, but susceptible to type-I and -II interferon.[45] In vivo, in studies using living cells, chikungunya virus appears to replicate in fibroblasts, skeletal muscle progenitor cells, and myofibers.[29][46][47]
The type-1 interferon response seems to play an important role in the host's response to chikungunya infection. Upon infection with chikungunya, the host's fibroblasts produce type-1 alpha and beta interferon (IFN-α and IFN-β).[46] In mouse studies, deficiencies in INF-1 in mice exposed to the virus cause increased morbidity and mortality.[46][48][49] The chikungunya-specific upstream components of the type-1 interferon pathway involved in the host's response to chikungunya infection are still unknown.[50] Nonetheless, mouse studies suggest that IPS-1 is an important factor,[50] and that IRF3 and IRF7 are important in an age-dependent manner.[51][52] Mouse studies also suggest that chikungunya evades host defenses and counters the type-I interferon response by producing NS2, a nonstructural protein that degrades RBP1 and turns off the host cell's ability to transcribe DNA.[53] NS2 interferes with the JAK-STAT signaling pathway and prevents STAT from becoming phosphorylated.[54]
In the acute phase of chikungunya, the virus is typically present in the areas where symptoms present, specifically skeletal muscles, and joints. In the chronic phase, it is suggested that viral persistence (the inability of the body to entirely rid itself of the virus), lack of clearance of the antigen, or both, contribute to joint pain. The inflammation response during both the acute and chronic phase of the disease results in part from interactions between the virus and monocytes and macrophages.[12] Chikungunya virus disease in humans is associated with elevated serum levels of specific cytokines and chemokines. High levels of specific cytokines have been linked to more severe acute disease: interleukin-6 (IL-6), IL-1β, RANTES, monocyte chemoattractant protein 1 (MCP-1), monokine induced by gamma interferon (MIG), and interferon gamma-induced protein 10 (IP-10). Cytokines may also contribute to chronic Chikungunya virus disease, as persistent joint pain has been associated with elevated levels of IL-6 and granulocyte-macrophage colony-stimulating factor (GM-CSF).[39] In those with chronic symptoms, a mild elevation of C-reactive protein (CRP) has been observed, suggesting ongoing chronic inflammation.[55]
Viral replication
The virus consists of four nonstructural proteins and three structural proteins.[12]
The structural proteins are the capsid and two envelope glycoproteins: E1 and E2, which form heterodimeric spikes on the viron surface. E2 binds to cellular receptors in order to enter the host cell through receptor-mediated endocytosis. E1 contains a fusion peptide which, when exposed to the acidity of the endosome in eukaryotic cells, dissociates from E2 and initiates membrane fusion that allows the release of nucleocapsids into the host cytoplasm, promoting infection.[56]
The mature virion contains 240 heterodimeric spikes of E2/E1, which after release, bud on the surface of the infected cell, where they are released by exocytosis to infect other cells.[35]
Diagnosis
Chikungunya is diagnosed on the basis of clinical, epidemiological, and laboratory criteria. Clinically, acute onset of high fever and severe joint pain would lead to suspicion of chikungunya. Epidemiological criteria consist of whether the individual has traveled to or spent time in an area in which chikungunya is present within the last twelve days (i.e.) the potential incubation period). Laboratory criteria include a decreased lymphocyte count consistent with viremia. However a definitive laboratory diagnosis can be accomplished through viral isolation, RT-PCR, or serological diagnosis.[57]
The differential diagnosis may include other mosquito-borne diseases, such as dengue or malaria, or other infections such as influenza. Chronic recurrent polyarthralgia occurs in at least 20% of chikungunya patients one year after infection, whereas such symptoms are uncommon in dengue.[58]
Virus isolation provides the most definitive diagnosis, but takes one to two weeks for completion and must be carried out in biosafety level III laboratories.[59] The technique involves exposing specific cell lines to samples from whole blood and identifying Chikungunya virus-specific responses. RT-PCR using nested primer pairs is used to amplify several chikungunya-specific genes from whole blood, generating thousands to millions of copies of the genes in order to identify them. RT-PCR can also be used to quantify the viral load in the blood. Using RT-PCR, diagnostic results can be available in one to two days.[59] Serological diagnosis requires a larger amount of blood than the other methods, and uses an ELISA assay to measure chikungunya-specific IgM levels in the blood serum. One advantage offered by serological diagnosis is that serum IgM is detectable from 5 days to months after the onset of symptoms, but drawbacks are that results may require two to three days, and false positives can occur with infection due to other related viruses, such as o'nyong'nyong virus and Semliki Forest virus.[59]
Presently, there is no specific way to test for chronic signs and symptoms associated with Chikungunya fever although nonspecific laboratory findings such as C reactive protein and elevated cytokines can correlate with disease activity.[60]
Prevention

Because no approved vaccine exists, the most effective means of prevention are protection against contact with the disease-carrying mosquitoes and controlling mosquito populations by limiting their habitat.[4] Mosquito control focuses on eliminating the standing water where mosquitos lay eggs and develop as larva; if elimination of the standing water is not possible, insecticides or biological control agents can be added.[12] Methods of protection against contact with mosquitos include using insect repellents with substances such as DEET, icaridin, PMD , or ethyl butylacetylaminopropionate.[61][62]
Wearing bite-proof long sleeves and trousers also offers protection, and garments can be treated with pyrethroids, a class of insecticides that often has repellent properties. Vaporized pyrethroids are also insect repellents. As infected mosquitoes often feed and rest inside homes, securing screens on windows and doors will help to keep mosquitoes out of the house.[61][62][63]
Vaccine
As of 2017, no approved vaccines are available. A phase-II vaccine trial used a live, attenuated virus, to develop viral resistance in 98% of those tested after 28 days and 85% still showed resistance after one year.[64] However, 8% of people reported transient joint pain, and attenuation was found to be due to only two mutations in the E2 glycoprotein.[65] Alternative vaccine strategies have been developed, and show efficacy in mouse models.[66][67] In August 2014 researchers at the National Institute of Allergy and Infectious Diseases in the USA were testing an experimental vaccine which uses virus-like particles (VLPs) instead of attenuated virus. All the 25 people participated in this phase 1 trial developed strong immune responses.[68] As of 2015, a phase 2 trial was planned, using 400 adults aged 18 to 60 and to take place at 6 locations in the Caribbean.[69] Even with a vaccine, mosquito population control and bite prevention will be necessary to control chikungunya disease.[70]
Treatment

Currently, no specific treatment for chikungunya is available.[4] Supportive care is recommended, and symptomatic treatment of fever and joint swelling includes the use of nonsteroidal anti-inflammatory drugs such as naproxen, non-aspirin analgesics such as paracetamol (acetaminophen) and fluids.[4] Aspirin is not recommended due to the increased risk of bleeding.[71] Despite anti-inflammatory effects, corticosteroids are not recommended during the acute phase of disease, as they may cause immunosuppression and worsen infection.[11]
Passive immunotherapy has potential benefit in treatment of chikungunya. Studies in animals using passive immunotherapy have been effective, and clinical studies using passive immunotherapy in those particularly vulnerable to severe infection are currently in progress.[72] Passive immunotherapy involves administration of anti-CHIKV hyperimmune human intravenous antibodies (immunoglobulins) to those exposed to a high risk of chikungunya infection. No antiviral treatment for Chikungunya virus is currently available, though testing has shown several medications to be effective in vitro.[9]
Chronic arthritis
In those who have more than two weeks of arthritis, ribavirin may be useful.[4] The effect of chloroquine is not clear.[4] It does not appear to help acute disease, but tentative evidence indicates it might help those with chronic arthritis.[4] Steroids do not appear to be an effective treatment.[4] NSAIDs and simple analgesics can be used to provide partial symptom relief in most cases. Methotrexate, a drug used in the treatment of rheumatoid arthritis, has been shown to have benefit in treating inflammatory polyarthritis resulting from chikungunya, though the drug mechanism for improving viral arthritis is unclear.[20]
Prognosis
The mortality rate of chikungunya is slightly less than 1 in 1000.[73] Those over the age of 65, neonates, and those with underlying chronic medical problems are most likely to have severe complications.[39] Neonates are vulnerable as it is possible to vertically transmit chikungunya from mother to infant during delivery, which results in high rates of morbidity, as infants lack fully developed immune systems.[39] The likelihood of prolonged symptoms or chronic joint pain is increased with increased age and prior rheumatological disease.[23][24]
Epidemiology
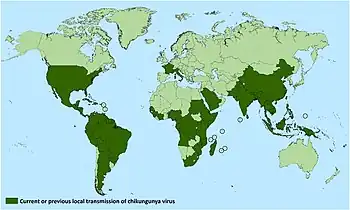

Dark blue: Native range
Teal: introduced
Historically, chikungunya has been present mostly in the developing world. The disease causes an estimated 3 million infections each year.[74] Epidemics in the Indian Ocean, Pacific Islands, and in the Americas, continue to change the distribution of the disease.[75] In Africa, chikungunya is spread by a sylvatic cycle in which the virus largely cycles between other non-human primates, small mammals, and mosquitos between human outbreaks.[10] During outbreaks, due to the high concentration of virus in the blood of those in the acute phase of infection, the virus can circulate from humans to mosquitoes and back to humans.[10] The transmission of the pathogen between humans and mosquitoes that exist in urban environments was established on multiple occasions from strains occurring on the eastern half of Africa in non-human primate hosts.[12] This emergence and spread beyond Africa may have started as early as the 18th century.[12] Currently, available data does not indicate whether the introduction of chikungunya into Asia occurred in the 19th century or more recently, but this epidemic Asian strain causes outbreaks in India and continues to circulate in Southeast Asia.[12] In Africa, outbreaks were typically tied to heavy rainfall causing increased mosquito population. In recent outbreaks in urban centers, the virus has spread by circulating between humans and mosquitoes.[11]
Global rates of chikungunya infection are variable, depending on outbreaks. When chikungunya was first identified in 1952, it had a low-level circulation in West Africa, with infection rates linked to rainfall. Beginning in the 1960s, periodic outbreaks were documented in Asia and Africa. However, since 2005, following several decades of relative inactivity, chikungunya has re-emerged and caused large outbreaks in Africa, Asia, and the Americas. In India, for instance, chikungunya re-appeared following 32 years of absence of viral activity.[76] Outbreaks have occurred in Europe, the Caribbean, and South America, areas in which chikungunya was not previously transmitted. Local transmission has also occurred in the United States and Australia, countries in which the virus was previously unknown.[11] In 2005, an outbreak on the island of Réunion was the largest then documented, with an estimated 266,000 cases on an island with a population of approximately 770,000.[77] In a 2006 outbreak, India reported 1.25 million suspected cases.[78] Chikungunya was recently introduced to the Americas, and from 2013 to 2014 in the Americas, 1,118,763 suspected cases and 24,682 confirmed cases were reported by the PAHO.[79]
An analysis of the genetic code of Chikungunya virus suggests that the increased severity of the 2005–present outbreak may be due to a change in the genetic sequence which altered the E1 segment of the virus' viral coat protein, a variant called E1-A226V. This mutation potentially allows the virus to multiply more easily in mosquito cells.[80] The change allows the virus to use the Asian tiger mosquito (an invasive species) as a vector in addition to the more strictly tropical main vector, Aedes aegypti.[81] Enhanced transmission of Chikungunya virus by A. albopictus could mean an increased risk for outbreaks in other areas where the Asian tiger mosquito is present.[82] A albopictus is an invasive species which has spread through Europe, the Americas, the Caribbean, Africa and the Middle East.[83]
After the detection of zika virus in Brazil in April 2015, the first ever in the Western Hemisphere,[84][85] it is now thought some chikungunya and dengue cases could in fact be zika virus cases or coinfections.
Outbreaks

2005 Réunion
The largest outbreak of chikungunya ever recorded at the time occurred on the island of Réunion in the western rim of the Indian Ocean from late March 2005 to February 2006.[86] At its height, the incidence peaked at about 25,000 cases per week or 3500 daily in early 2006. [87]
2007 Italy
In September 2007, 130 cases were confirmed in the province of Ravenna, Northern Italy, in the contiguous towns of Castiglione di Cervia and Castiglione di Ravenna. One person died. The source of the outbreak was an Indian from Kerala, India.[88]
2011–15 Pacific Islands
Outbreaks in the Pacific Islands began in New Caledonia in 2011 and have since occurred in a number of Pacific countries.[89][90]
2014 United States
On July 17, 2014, the first chikungunya case acquired in the United States was reported in Florida by the Centers for Disease Control and Prevention in a man who had not recently traveled outside the United States.[91]
2014 Mexico
On 7 November 2014 Mexico reported an outbreak of chikungunya, acquired by local transmission, in southern state of Chiapas. The outbreak extends across the coastline from the Guatemala border to the neighbouring state of Oaxaca. Health authorities have reported a cumulative load of 39 laboratory-confirmed cases (by the end of week 48). No suspect cases have been reported.[92]
2000 India
A outbreak of chikungunya fever was reported from Malegaon town in Nasik district, Maharashtra state, in the first two weeks of March 2006, resulting in over 2000 cases. In Orissa state, at most 5000 cases of fever with muscle aches and headache were reported between February 27 and March 5, 2006.[93]
History
The word 'chikungunya' is believed to have been derived from a description in the Makonde language, meaning "that which bends up", of the contorted posture of people affected with the severe joint pain and arthritic symptoms associated with this disease.[94] The disease was first described by Marion Robinson[95] and W.H.R. Lumsden[96] in 1955, following an outbreak in 1952 on the Makonde Plateau.
According to the initial 1955 report about the epidemiology of the disease, the term 'chikungunya' is derived from the Makonde root verb kungunyala, meaning to dry up or become contorted. In concurrent research, Robinson glossed the Makonde term more specifically as "that which bends up". Subsequent authors apparently overlooked the references to the Makonde language and assumed the term to have been derived from Swahili, the lingua franca of the region. The erroneous attribution to Swahili has been repeated in numerous print sources.[97]
Since its discovery in Tanganyika, Africa, in 1952, Chikungunya virus outbreaks have occurred occasionally in Africa, South Asia, and Southeast Asia, but recent outbreaks have spread the disease over a wider range.[98]
The first recorded outbreak of this disease may have been in 1779.[99] This is in agreement with the molecular genetics evidence that suggests it evolved around the year 1700.[100]
Society and culture
Chikungunya is one of more than a dozen agents researched as a potential biological weapon.[101]
Research
This disease is part of the group of neglected tropical diseases.[102]
See also
References
- ↑ "chikungunya". Oxford Learner's Dictionary. Oxford University Press. Archived from the original on 4 November 2014. Retrieved 4 November 2014.
- 1 2 3 4 5 6 7 8 9 "Chikungunya Virus Symptoms, Diagnosis, & Treatment". CDC. 6 April 2016. Archived from the original on 21 September 2016. Retrieved 26 September 2016.
- 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 "Chikungunya Fact sheet". WHO. April 2016. Archived from the original on 27 September 2016. Retrieved 26 September 2016.
- 1 2 3 4 5 6 7 8 9 10 11 12 Caglioti C, Lalle E, Castilletti C, Carletti F, Capobianchi MR, Bordi L (July 2013). "Chikungunya virus infection: an overview". The New Microbiologica. 36 (3): 211–27. PMID 23912863.
- ↑ van Aalst M, Nelen CM, Goorhuis A, Stijnis C, Grobusch MP (January 2017). "Long-term sequelae of chikungunya virus disease: A systematic review". Travel Medicine and Infectious Disease. 15: 8–22. doi:10.1016/j.tmaid.2017.01.004. PMID 28163198.
- ↑ "Prevention". CDC. 26 February 2016. Archived from the original on 15 September 2016. Retrieved 26 September 2016.
- ↑ Staples JE, Fischer M (September 2014). "Chikungunya virus in the Americas--what a vectorborne pathogen can do". The New England Journal of Medicine. 371 (10): 887–9. doi:10.1056/NEJMp1407698. PMC 4624217. PMID 25184860.
- ↑ "2016 provisional data for the United States". CDC. 20 September 2016. Archived from the original on 18 September 2016. Retrieved 26 September 2016.
- 1 2 3 4 5 6 7 8 9 Thiberville SD, Moyen N, Dupuis-Maguiraga L, Nougairede A, Gould EA, Roques P, de Lamballerie X (September 2013). "Chikungunya fever: epidemiology, clinical syndrome, pathogenesis and therapy". Antiviral Research. 99 (3): 345–70. doi:10.1016/j.antiviral.2013.06.009. PMC 7114207. PMID 23811281.
{{cite journal}}: CS1 maint: url-status (link) - 1 2 3 4 5 Powers AM, Logue CH (September 2007). "Changing patterns of chikungunya virus: re-emergence of a zoonotic arbovirus". The Journal of General Virology. 88 (Pt 9): 2363–77. doi:10.1099/vir.0.82858-0. PMID 17698645.
- 1 2 3 4 5 6 7 8 9 Burt FJ, Rolph MS, Rulli NE, Mahalingam S, Heise MT (February 2012). "Chikungunya: a re-emerging virus". Lancet. 379 (9816): 662–71. doi:10.1016/S0140-6736(11)60281-X. PMID 22100854. S2CID 33440699.
- 1 2 3 4 5 6 7 8 9 Weaver SC, Lecuit M (March 2015). "Chikungunya virus and the global spread of a mosquito-borne disease". The New England Journal of Medicine. 372 (13): 1231–9. doi:10.1056/NEJMra1406035. PMID 25806915.
- ↑ Chhabra M, Mittal V, Bhattacharya D, Rana U, Lal S (2008). "Chikungunya fever: a re-emerging viral infection". Indian Journal of Medical Microbiology (Submitted manuscript). 26 (1): 5–12. doi:10.4103/0255-0857.38850. PMID 18227590. Archived from the original on 25 June 2020. Retrieved 29 July 2020.
- ↑ Capeding MR, Chua MN, Hadinegoro SR, Hussain II, Nallusamy R, Pitisuttithum P, et al. (2013). "Dengue and other common causes of acute febrile illness in Asia: an active surveillance study in children". PLOS Neglected Tropical Diseases. 7 (7): e2331. doi:10.1371/journal.pntd.0002331. PMC 3723539. PMID 23936565.

- ↑ KUMAR, DR MUNEESH; DEVI, DR SANGEETA (26 January 2021). A TEXTBOOK OF VECTOR BORNE DISEASES. Darshan Publishers. p. 18. ISBN 978-93-86739-10-0. Archived from the original on 2 July 2022. Retrieved 1 July 2022.
- ↑ Powers, Ann. "Chikungunya". CDC. Archived from the original on 27 February 2014. Retrieved 12 May 2014.
- ↑ Mahendradas P, Ranganna SK, Shetty R, Balu R, Narayana KM, Babu RB, Shetty BK (February 2008). "Ocular manifestations associated with chikungunya". Ophthalmology. 115 (2): 287–91. doi:10.1016/j.ophtha.2007.03.085. PMID 17631967.
- ↑ Simon F, Javelle E, Oliver M, Leparc-Goffart I, Marimoutou C (June 2011). "Chikungunya virus infection". Current Infectious Disease Reports. 13 (3): 218–28. doi:10.1007/s11908-011-0180-1. PMC 3085104. PMID 21465340.
- ↑ MacFadden DR, Bogoch II (July 2014). "Chikungunya". CMAJ. 186 (10): 775. doi:10.1503/cmaj.140031. PMC 4081202. PMID 24914111.
- 1 2 Parashar D, Cherian S (2014). "Antiviral perspectives for chikungunya virus". BioMed Research International. 2014: 631642. doi:10.1155/2014/631642. PMC 4052087. PMID 24955364.
- ↑ Javelle E, Ribera A, Degasne I, Gaüzère BA, Marimoutou C, Simon F (March 2015). "Specific management of post-chikungunya rheumatic disorders: a retrospective study of 159 cases in Reunion Island from 2006-2012". PLOS Neglected Tropical Diseases. 9 (3): e0003603. doi:10.1371/journal.pntd.0003603. PMC 4356515. PMID 25760632.
- ↑ Fourie ED, Morrison JG (July 1979). "Rheumatoid arthritic syndrome after chikungunya fever". South African Medical Journal = Suid-Afrikaanse Tydskrif vir Geneeskunde. 56 (4): 130–2. PMID 494034.
- 1 2 3 4 Schilte C, Staikowsky F, Staikovsky F, Couderc T, Madec Y, Carpentier F, et al. (2013). "Chikungunya virus-associated long-term arthralgia: a 36-month prospective longitudinal study". PLOS Neglected Tropical Diseases. 7 (3): e2137. doi:10.1371/journal.pntd.0002137. PMC 3605278. PMID 23556021.
- 1 2 3 Gérardin P, Fianu A, Michault A, Mussard C, Boussaïd K, Rollot O, et al. (January 2013). "Predictors of Chikungunya rheumatism: a prognostic survey ancillary to the TELECHIK cohort study". Arthritis Research & Therapy. 15 (1): R9. doi:10.1186/ar4137. PMC 3672753. PMID 23302155.
- 1 2 Moro ML, Grilli E, Corvetta A, Silvi G, Angelini R, Mascella F, et al. (August 2012). "Long-term chikungunya infection clinical manifestations after an outbreak in Italy: a prognostic cohort study". The Journal of Infection. 65 (2): 165–72. doi:10.1016/j.jinf.2012.04.005. PMID 22522292.
- ↑ Sissoko D, Malvy D, Ezzedine K, Renault P, Moscetti F, Ledrans M, Pierre V (2009). "Post-epidemic Chikungunya disease on Reunion Island: course of rheumatic manifestations and associated factors over a 15-month period". PLOS Neglected Tropical Diseases. 3 (3): e389. doi:10.1371/journal.pntd.0000389. PMC 2647734. PMID 19274071.
- ↑ Larrieu S, Pouderoux N, Pistone T, Filleul L, Receveur MC, Sissoko D, et al. (January 2010). "Factors associated with persistence of arthralgia among Chikungunya virus-infected travellers: report of 42 French cases". Journal of Clinical Virology. 47 (1): 85–8. doi:10.1016/j.jcv.2009.11.014. PMID 20004145.
- ↑ Manimunda SP, Vijayachari P, Uppoor R, Sugunan AP, Singh SS, Rai SK, et al. (June 2010). "Clinical progression of chikungunya fever during acute and chronic arthritic stages and the changes in joint morphology as revealed by imaging". Transactions of the Royal Society of Tropical Medicine and Hygiene. 104 (6): 392–9. doi:10.1016/j.trstmh.2010.01.011. PMID 20171708.
- 1 2 Ozden S, Huerre M, Riviere JP, Coffey LL, Afonso PV, Mouly V, et al. (June 2007). "Human muscle satellite cells as targets of Chikungunya virus infection". PLOS ONE. 2 (6): e527. Bibcode:2007PLoSO...2..527O. doi:10.1371/journal.pone.0000527. PMC 1885285. PMID 17565380.
- ↑ Hoarau JJ, Jaffar Bandjee MC, Krejbich Trotot P, Das T, Li-Pat-Yuen G, Dassa B, et al. (May 2010). "Persistent chronic inflammation and infection by Chikungunya arthritogenic alphavirus in spite of a robust host immune response". Journal of Immunology. 184 (10): 5914–27. doi:10.4049/jimmunol.0900255. PMID 20404278.
- ↑ Hawman DW, Stoermer KA, Montgomery SA, Pal P, Oko L, Diamond MS, Morrison TE (December 2013). "Chronic joint disease caused by persistent Chikungunya virus infection is controlled by the adaptive immune response". Journal of Virology. 87 (24): 13878–88. doi:10.1128/JVI.02666-13. PMC 3838294. PMID 24131709.
- ↑ Teo TH, Lum FM, Claser C, Lulla V, Lulla A, Merits A, et al. (January 2013). "A pathogenic role for CD4+ T cells during Chikungunya virus infection in mice". Journal of Immunology. 190 (1): 259–69. doi:10.4049/jimmunol.1202177. PMID 23209328.
- ↑ Labadie K, Larcher T, Joubert C, Mannioui A, Delache B, Brochard P, et al. (March 2010). "Chikungunya disease in nonhuman primates involves long-term viral persistence in macrophages". The Journal of Clinical Investigation. 120 (3): 894–906. doi:10.1172/JCI40104. PMC 2827953. PMID 20179353.
- ↑ Sun S, Xiang Y, Akahata W, Holdaway H, Pal P, Zhang X, et al. (April 2013). "Structural analyses at pseudo atomic resolution of Chikungunya virus and antibodies show mechanisms of neutralization". eLife. 2: e00435. doi:10.7554/eLife.00435. PMC 3614025. PMID 23577234.
- 1 2 Weaver SC, Osorio JE, Livengood JA, Chen R, Stinchcomb DT (September 2012). "Chikungunya virus and prospects for a vaccine". Expert Review of Vaccines. 11 (9): 1087–101. doi:10.1586/erv.12.84. PMC 3562718. PMID 23151166.
- ↑ Powers AM, Brault AC, Shirako Y, Strauss EG, Kang W, Strauss JH, Weaver SC (November 2001). "Evolutionary relationships and systematics of the alphaviruses". Journal of Virology. 75 (21): 10118–31. doi:10.1128/JVI.75.21.10118-10131.2001. PMC 114586. PMID 11581380.
- ↑ "NIAID Category A, B, and C Priority Pathogens". Archived from the original on 5 January 2014. Retrieved 23 July 2020.
- ↑ "Biosafety in Microbiological and Biomedical Laboratories (BMBL) Fifth Edition" (PDF). Archived (PDF) from the original on 14 October 2014. Retrieved 1 January 2014.
- 1 2 3 4 Morrison TE (October 2014). "Reemergence of chikungunya virus". Journal of Virology. 88 (20): 11644–7. doi:10.1128/JVI.01432-14. PMC 4178719. PMID 25078691.
- ↑ Ng LC, Hapuarachchi HC (October 2010). "Tracing the path of Chikungunya virus--evolution and adaptation". Infection, Genetics and Evolution. 10 (7): 876–85. doi:10.1016/j.meegid.2010.07.012. PMID 20654736.
- ↑ Powers AM, Brault AC, Tesh RB, Weaver SC (February 2000). "Re-emergence of Chikungunya and O'nyong-nyong viruses: evidence for distinct geographical lineages and distant evolutionary relationships". The Journal of General Virology. 81 (Pt 2): 471–9. doi:10.1099/0022-1317-81-2-471. PMID 10644846.
- ↑ Sahadeo NS, Allicock OM, De Salazar PM, Auguste AJ, Widen S, Olowokure B, Gutierrez C, Valadere AM, Polson-Edwards K, Weaver SC, Carrington CV (2017). "Understanding the evolution and spread of chikungunya virus in the Americas using complete genome sequences". Virus Evol. 3. doi:10.1093/ve/vex010.
{{cite journal}}: CS1 maint: multiple names: authors list (link) - ↑ Sahadeo, N. S. D.; Allicock, O. M.; De Salazar, P. M.; Auguste, A. J.; Widen, S.; Olowokure, B.; Gutierrez, C.; Valadere, A. M.; Polson-Edwards, K.; Weaver, S. C.; Carrington, C. V. F. (January 2017). "Understanding the evolution and spread of chikungunya virus in the Americas using complete genome sequences". Virus Evolution. 3 (1): vex010. doi:10.1093/ve/vex010. ISSN 2057-1577. Archived from the original on 16 June 2022. Retrieved 7 July 2022.
- ↑ Enserink M (September 2007). "Epidemiology. Tropical disease follows mosquitoes to Europe". Science. 317 (5844): 1485. doi:10.1126/science.317.5844.1485a. PMID 17872417. S2CID 83359245.
- ↑ Sourisseau M, Schilte C, Casartelli N, Trouillet C, Guivel-Benhassine F, Rudnicka D, et al. (June 2007). "Characterization of reemerging chikungunya virus". PLOS Pathogens. 3 (6): e89. doi:10.1371/journal.ppat.0030089. PMC 1904475. PMID 17604450.
- 1 2 3 Schilte C, Couderc T, Chretien F, Sourisseau M, Gangneux N, Guivel-Benhassine F, et al. (February 2010). "Type I IFN controls chikungunya virus via its action on nonhematopoietic cells". The Journal of Experimental Medicine. 207 (2): 429–42. doi:10.1084/jem.20090851. PMC 2822618. PMID 20123960.
- ↑ Rohatgi A, Corbo JC, Monte K, Higgs S, Vanlandingham DL, Kardon G, Lenschow DJ (March 2014). "Infection of myofibers contributes to increased pathogenicity during infection with an epidemic strain of chikungunya virus". Journal of Virology. 88 (5): 2414–25. doi:10.1128/JVI.02716-13. PMC 3958092. PMID 24335291.
- ↑ Couderc T, Chrétien F, Schilte C, Disson O, Brigitte M, Guivel-Benhassine F, et al. (February 2008). "A mouse model for Chikungunya: young age and inefficient type-I interferon signaling are risk factors for severe disease". PLOS Pathogens. 4 (2): e29. doi:10.1371/journal.ppat.0040029. PMC 2242832. PMID 18282093.
- ↑ Partidos CD, Weger J, Brewoo J, Seymour R, Borland EM, Ledermann JP, et al. (April 2011). "Probing the attenuation and protective efficacy of a candidate chikungunya virus vaccine in mice with compromised interferon (IFN) signaling". Vaccine. 29 (16): 3067–73. doi:10.1016/j.vaccine.2011.01.076. PMC 3081687. PMID 21300099.
- 1 2 White LK, Sali T, Alvarado D, Gatti E, Pierre P, Streblow D, Defilippis VR (January 2011). "Chikungunya virus induces IPS-1-dependent innate immune activation and protein kinase R-independent translational shutoff". Journal of Virology. 85 (1): 606–20. doi:10.1128/JVI.00767-10. PMC 3014158. PMID 20962078.
- ↑ Rudd PA, Wilson J, Gardner J, Larcher T, Babarit C, Le TT, et al. (September 2012). "Interferon response factors 3 and 7 protect against Chikungunya virus hemorrhagic fever and shock". Journal of Virology. 86 (18): 9888–98. doi:10.1128/JVI.00956-12. PMC 3446587. PMID 22761364.
- ↑ Schilte C, Buckwalter MR, Laird ME, Diamond MS, Schwartz O, Albert ML (April 2012). "Cutting edge: independent roles for IRF-3 and IRF-7 in hematopoietic and nonhematopoietic cells during host response to Chikungunya infection". Journal of Immunology. 188 (7): 2967–71. doi:10.4049/jimmunol.1103185. PMID 22371392.
- ↑ Akhrymuk I, Kulemzin SV, Frolova EI (July 2012). "Evasion of the innate immune response: the Old World alphavirus nsP2 protein induces rapid degradation of Rpb1, a catalytic subunit of RNA polymerase II". Journal of Virology. 86 (13): 7180–91. doi:10.1128/JVI.00541-12. PMC 3416352. PMID 22514352.
- ↑ Fros JJ, Liu WJ, Prow NA, Geertsema C, Ligtenberg M, Vanlandingham DL, et al. (October 2010). "Chikungunya virus nonstructural protein 2 inhibits type I/II interferon-stimulated JAK-STAT signaling". Journal of Virology. 84 (20): 10877–87. doi:10.1128/JVI.00949-10. PMC 2950581. PMID 20686047.
- ↑ Nehring, Sara M.; Goyal, Amandeep; Patel, Bhupendra C. (2022). "C Reactive Protein". StatPearls. StatPearls Publishing. Archived from the original on 17 June 2022. Retrieved 3 July 2022."More than 10.0 mg/L: Marked elevation (Acute bacterial infections, viral infections, systemic vasculitis, major trauma)."
- ↑ Voss JE, Vaney MC, Duquerroy S, Vonrhein C, Girard-Blanc C, Crublet E, et al. (December 2010). "Glycoprotein organization of Chikungunya virus particles revealed by X-ray crystallography". Nature. 468 (7324): 709–12. Bibcode:2010Natur.468..709V. doi:10.1038/nature09555. PMID 21124458. S2CID 4412764.
- ↑ Cabié A, Ledrans M, Abel S (July 2015). "Chikungunya Virus Infections". The New England Journal of Medicine. 373 (1): 94. doi:10.1056/NEJMc1505501. PMID 26132958.
- ↑ Morens DM, Fauci AS (September 2014). "Chikungunya at the door--déjà vu all over again?". The New England Journal of Medicine. 371 (10): 885–7. doi:10.1056/NEJMp1408509. PMID 25029435.
- 1 2 3 "Laboratory Diagnosis of Chikungunya Fevers". World Health Organization. Archived from the original on 8 September 2012. Retrieved 20 May 2013.
- ↑ Schilte C, Staikowsky F, Staikovsky F, Couderc T, Madec Y, Carpentier F, et al. (2013). "Chikungunya virus-associated long-term arthralgia: a 36-month prospective longitudinal study". PLOS Neglected Tropical Diseases. 7 (3): e2137. doi:10.1371/journal.pntd.0002137. PMC 3605278. PMID 23556021.
- 1 2 "Prevention | Chikungunya virus | CDC". www.cdc.gov. 10 June 2022. Archived from the original on 15 September 2016. Retrieved 4 July 2022.
- 1 2 "Guidelines for prevention and control of Chikungunya fever". www.who.int. Archived from the original on 8 July 2022. Retrieved 5 July 2022.
- ↑ Vu, David M.; Jungkind, Donald; Angelle Desiree LaBeaud, null (June 2017). "Chikungunya Virus". Clinics in Laboratory Medicine. 37 (2): 371–382. doi:10.1016/j.cll.2017.01.008. ISSN 1557-9832. Archived from the original on 20 March 2022. Retrieved 10 July 2022.
- ↑ Edelman R, Tacket CO, Wasserman SS, Bodison SA, Perry JG, Mangiafico JA (June 2000). "Phase II safety and immunogenicity study of live chikungunya virus vaccine TSI-GSD-218". The American Journal of Tropical Medicine and Hygiene. 62 (6): 681–5. doi:10.4269/ajtmh.2000.62.681. PMID 11304054.
- ↑ Gorchakov R, Wang E, Leal G, Forrester NL, Plante K, Rossi SL, et al. (June 2012). "Attenuation of Chikungunya virus vaccine strain 181/clone 25 is determined by two amino acid substitutions in the E2 envelope glycoprotein". Journal of Virology. 86 (11): 6084–96. doi:10.1128/JVI.06449-11. PMC 3372191. PMID 22457519.
- ↑ Plante K, Wang E, Partidos CD, Weger J, Gorchakov R, Tsetsarkin K, et al. (July 2011). "Novel chikungunya vaccine candidate with an IRES-based attenuation and host range alteration mechanism". PLOS Pathogens. 7 (7): e1002142. doi:10.1371/journal.ppat.1002142. PMC 3145802. PMID 21829348.
- ↑ Hallengärd D, Kakoulidou M, Lulla A, Kümmerer BM, Johansson DX, Mutso M, et al. (March 2014). "Novel attenuated Chikungunya vaccine candidates elicit protective immunity in C57BL/6 mice". Journal of Virology. 88 (5): 2858–66. doi:10.1128/JVI.03453-13. PMC 3958085. PMID 24371047.
- ↑ "Experimental chikungunya vaccine passes first test". NPR. 15 August 2014. Archived from the original on 19 August 2014. Retrieved 15 August 2014.
- ↑ Al Idrus, Amirah (2 December 2015). "NIAID to bring Chikungunya vaccine into Phase II". fiercevaccines.com. Archived from the original on 10 April 2016. Retrieved 24 March 2016.
- ↑ Morens DM, Fauci AS (September 2014). "Chikungunya at the door--déjà vu all over again?". The New England Journal of Medicine. 371 (10): 885–7. doi:10.1056/nejmp1408509. PMID 25029435.
- ↑ "Chikungunya—Fact sheet". European Centre for Disease Prevention and Control (ECDC). Archived from the original on 19 December 2013. Retrieved 17 December 2013.
- ↑ Couderc T, Khandoudi N, Grandadam M, Visse C, Gangneux N, Bagot S, et al. (August 2009). "Prophylaxis and therapy for Chikungunya virus infection". The Journal of Infectious Diseases. 200 (4): 516–23. doi:10.1086/600381. PMID 19572805.
- ↑ Mavalankar D, Shastri P, Bandyopadhyay T, Parmar J, Ramani KV (March 2008). "Increased mortality rate associated with chikungunya epidemic, Ahmedabad, India". Emerging Infectious Diseases. 14 (3): 412–5. doi:10.3201/eid1403.070720. PMC 2570824. PMID 18325255.
- ↑ Seppa, Nathan (2 June 2015). "Chikungunya is on the move". Science News. Archived from the original on 11 June 2015. Retrieved 13 June 2015.
- ↑ Sam IC, Loong SK, Michael JC, Chua CL, Wan Sulaiman WY, Vythilingam I, et al. (2012). "Genotypic and phenotypic characterization of Chikungunya virus of different genotypes from Malaysia". PLOS ONE. 7 (11): e50476. Bibcode:2012PLoSO...750476S. doi:10.1371/journal.pone.0050476. PMC 3507689. PMID 23209750.
- ↑ Lahariya C, Pradhan SK (December 2006). "Emergence of chikungunya virus in Indian subcontinent after 32 years: A review" (PDF). Journal of Vector Borne Diseases. 43 (4): 151–60. PMID 17175699. Archived from the original (PDF) on 19 October 2013.
- ↑ Roth A, Hoy D, Horwood PF, Ropa B, Hancock T, Guillaumot L, et al. (August 2014). "Preparedness for threat of chikungunya in the pacific". Emerging Infectious Diseases. 20 (8). doi:10.3201/eid2008.130696. PMC 4111160. PMID 25062306.
- ↑ Muniaraj M (March 2014). "Fading chikungunya fever from India: beginning of the end of another episode?". The Indian Journal of Medical Research. 139 (3): 468–70. PMC 4069744. PMID 24820844.
- ↑ "Number of cumulative cases 2013–2014". www.paho.org. Pan-American Health Organization (PAHO). 15 May 2015. Archived from the original on 21 July 2015. Retrieved 19 July 2015.
- ↑ Schuffenecker I, Iteman I, Michault A, Murri S, Frangeul L, Vaney MC, et al. (July 2006). "Genome microevolution of chikungunya viruses causing the Indian Ocean outbreak". PLOS Medicine. 3 (7): e263. doi:10.1371/journal.pmed.0030263. PMC 1463904. PMID 16700631.
- ↑ Tsetsarkin KA, Vanlandingham DL, McGee CE, Higgs S (December 2007). "A single mutation in chikungunya virus affects vector specificity and epidemic potential". PLOS Pathogens. 3 (12): e201. doi:10.1371/journal.ppat.0030201. PMC 2134949. PMID 18069894.
- ↑ Liumbruno GM, Calteri D, Petropulacos K, Mattivi A, Po C, Macini P, et al. (October 2008). "The Chikungunya epidemic in Italy and its repercussion on the blood system". Blood Transfusion = Trasfusione del Sangue. 6 (4): 199–210. doi:10.2450/2008.0016-08. PMC 2626913. PMID 19112735.
- ↑ Gratz, N. G. (September 2004). "Critical review of the vector status of Aedes albopictus". Medical and Veterinary Entomology. 18 (3): 215–227. doi:10.1111/j.0269-283X.2004.00513.x. Archived from the original on 24 June 2022. Retrieved 3 July 2022.
- ↑ "Identificado vírus causador de doença misteriosa em Salvador e RMS". 29 April 2015. Archived from the original on 18 May 2015. Retrieved 9 May 2015.
- ↑ "Archived copy". Archived from the original on 5 May 2015. Retrieved 9 May 2015.
{{cite web}}: CS1 maint: archived copy as title (link) - ↑ "PRO/EDR> Chikungunya - Mauritius and Reunion Island (09): Reunion 2006-02-14 23:50:00 Archive Number: 20060214.0491". ProMED Mail. Archived from the original on 24 September 2015. Retrieved 30 June 2022.
- ↑ "PRO/EDR> Chikungunya - Mauritius and Reunion Island (04): Reunion 2006-01-27 23:50:00 Archive Number: 20060127.0254". ProMED Mail. Archived from the original on 24 September 2015. Retrieved 30 June 2022.
- ↑ (7 September 2007) Chikungunya outbreak in Italy Health Protection Report, Volume 1, Number 36, UK NHS, Retrieved 23 March 2015
- ↑ Roth, A.; et al. (16 October 2014). "Concurrent outbreaks of dengue, chikungunya and Zika virus infections – an unprecedented epidemic wave of mosquito-borne viruses in the Pacific 2012–2014". Eurosurveillance. 19 (41). doi:10.2807/1560-7917.ES2014.19.41.20929. PMID 25345518. Archived from the original on 26 January 2015. Retrieved 14 February 2015.
- ↑ "Chikungunya virus: Pacific Islands (Samoa, American Samoa, Tonga, Tokelau and French Polynesia)". National Travel Health Network and Centre. 17 October 2014. Archived from the original on 14 February 2015. Retrieved 14 February 2015.
- ↑ "First Chikungunya case acquired in the United States reported in Florida | Press Release | CDC Online Newsroom | CDC". Cdc.gov. 17 July 2014. Archived from the original on 26 January 2022. Retrieved 24 August 2014.
- ↑ Toribio, Laura (12 February 2014). "Se triplican los casos de Chikungunya en Chiapas". Excelsior (in español). InventMX. Archived from the original on 13 December 2014. Retrieved 3 December 2014.
En una semana, los casos confirmados del virus pasaron de 14 a 39 en el estado, informó el subsecretario de Prevención y Promoción de la Salud de la Secretaría de Salud, Pablo Kuri Morales.
- ↑ "MD Travel Health—India—vaccinations, malaria, safety, and other medical advice". MDtravelhealth.com. Archived from the original on 5 August 2014. Retrieved 23 May 2014.
- ↑ Centers for Disease Control Prevention (CDC) (September 2006). "Chikungunya fever diagnosed among international travelers--United States, 2005-2006". MMWR. Morbidity and Mortality Weekly Report. 55 (38): 1040–2. PMID 17008866. Archived from the original on 28 May 2017.
- ↑ Robinson MC (January 1955). "An epidemic of virus disease in Southern Province, Tanganyika Territory, in 1952-53. I. Clinical features". Transactions of the Royal Society of Tropical Medicine and Hygiene. 49 (1): 28–32. doi:10.1016/0035-9203(55)90080-8. PMID 14373834.
- ↑ Lumsden WH (January 1955). "An epidemic of virus disease in Southern Province, Tanganyika Territory, in 1952-53. II. General description and epidemiology". Transactions of the Royal Society of Tropical Medicine and Hygiene. 49 (1): 33–57. doi:10.1016/0035-9203(55)90081-X. PMID 14373835.
- ↑ Benjamin M (2008). "Chikungunya is NOT a Swahili word, it is from the Makonde language!".
{{cite web}}: CS1 maint: url-status (link) - ↑ Peterson, Phillip K. (8 August 2020). Microbes: The Life-Changing Story of Germs. Rowman & Littlefield. p. 258. ISBN 978-1-63388-635-3. Archived from the original on 8 July 2022. Retrieved 6 July 2022.
- ↑ Carey DE (July 1971). "Chikungunya and dengue: a case of mistaken identity?". Journal of the History of Medicine and Allied Sciences. 26 (3): 243–62. doi:10.1093/jhmas/XXVI.3.243. PMID 4938938.
- ↑ Cherian SS, Walimbe AM, Jadhav SM, Gandhe SS, Hundekar SL, Mishra AC, Arankalle VA (January 2009). "Evolutionary rates and timescale comparison of Chikungunya viruses inferred from the whole genome/E1 gene with special reference to the 2005-07 outbreak in the Indian subcontinent". Infection, Genetics and Evolution. 9 (1): 16–23. doi:10.1016/j.meegid.2008.09.004. PMID 18940268.
- ↑ "Chemical and Biological Weapons: Possession and Programs Past and Present Archived 23 June 2014 at the Wayback Machine", James Martin Center for Nonproliferation Studies, Middlebury College, 9 April 2002, accessed 18 June 2014.
- ↑ "Neglected tropical diseases". WHO. Archived from the original on 22 February 2014. Retrieved 26 September 2016.
Further reading
- "Snapshots capture self-assembly of dangerous virus". Nature: d41586–022–01847-0. 7 July 2022. doi:10.1038/d41586-022-01847-0. Archived from the original on 15 July 2022. Retrieved 9 July 2022.
External links
- Chikungunya fact sheet Archived 27 September 2016 at the Wayback Machine—from the World Health Organization (WHO)
- Chikungunya outbreaks Archived 15 July 2020 at the Wayback Machine—from the World Health Organization (WHO)
- "Chikungunya". European Centre for Disease Prevention and Control. 23 January 2008. Archived from the original on 5 August 2009. Retrieved 20 May 2013.
- Chikungunya in Cuba Archived 18 July 2014 at the Wayback Machine
- Chikungunya: The key role of "innate immunity"
| Classification | |
|---|---|
| External resources |
|