Delayed puberty
| Delayed puberty | |
|---|---|
| Video explanation | |
| Specialty | Endocrinology |
| Symptoms | Females: No breast development by 13, no menstruation by 16[1] Boys: No testicle enlargement by 14[1] |
| Complications | Short height, osteoporosis, psychological stress[2] |
| Types | Constitutional delay, functional hypogonadotropic hypogonadism, hypergonadotropic hypogonadism, permanent hypogonadotropic hypogonadism[3] |
| Causes | Family history, long term health problems, failure of the gonads, conditions affecting the hypothalamic pituitary gonadal axis[3] |
| Diagnostic method | FSH, LH, testosterone, estradiol, bone age X-rays[4] |
| Treatment | Depends on the underlying cause[3] |
| Frequency | ~2%[2] |
Delayed puberty is a lacks of or incomplete development of sexual characteristics past the usual age of onset of puberty.[3] In girls this is a lack of breast development by age 13 or not menstruating by age 16 while in boys it is the lack of testicle enlargement by age 14.[1] There may or may not be an absence of acne, pubic hair, and body odor.[1] Complications may include short height, osteoporosis, and psychological stress.[2]
The most common cause, known as constitutional delay, is a temporary delay that runs in families.[3] The next most common group is the result of long term health problems, like diabetes, anorexia, cystic fibrosis or malnutrition.[3] The third group is failure of the gonads, resulting in hypergonadotropic hypogonadism, which can occur due to undescended testicles, gonadal dysgenesis, chemotherapy, Turner syndrome, or Klinefelter syndrome.[3] The final group involves conditions that affect the hypothalamic pituitary gonadal axis such as Kallmann syndrome or brain tumors.[3][1] Diagnosis may involve measuring blood FSH, LH, and testosterone or estradiol, as well as bone age X-rays.[4]
Treatment is based on the underlying cause.[3] A constitutional delay may be managed by simple reassurance or with short term use of hormones.[3] People with long term problems are often treated with long-term hormone replacement, testosterone in males and estrogen with progesterone in females.[1] Outcomes depend on the underlying condition.[1]
Delayed puberty affects about 2% of adolescents.[2] Males are more commonly affected than females.[3] Constitutional delay is the cause of about 60% of cases in males and 30% of cases in girls.[4] While the average age of menstruation may have decreased since the 1800s,[5] the onset of other signs of puberty appears not to have changed much over time.[6]
Signs and symptoms


Puberty is considered delayed when the child has not begun puberty when two standard deviations or about 95% of children from similar backgrounds have.[7][8][9]
In North American girls, puberty is considered delayed when breast development has not begun by age 13, when they have not started menstruating by age 16,[3] and when there is no increased growth rate.[8] Furthermore, slowed progression through the Tanner scale or lack of menarche within 3 years of breast development may also be considered delayed puberty.[8]
In the United States, the age of onset of puberty in girls depends on racial background. Delayed puberty means the lack of breast development by age 12.8 years for White girls, and by age 12.4 years for Black girls.[7][8] The lack of menstruation by age 15 in any ethnic background is considered delayed.[8]
In North American boys, puberty is considered delayed when the testes remain less than 2.5 cm in diameter[3] or less than 4 mL in volume by the age of 14.[4] Delayed puberty is more common in males.[3]
Although absence of pubic or armput hair is common in children with delayed puberty, the presence of sexual hair is due to adrenal sex hormone secretion unrelated to the sex hormones produced by the ovaries or testes.[10][8]
The age of onset of puberty is dependent on genetics, general health, socioeconomic status, and environmental exposures. Children residing closer to the equator, at lower altitudes, in cities and other urban areas generally begin the process of puberty earlier than their counterparts.[7] Mildly obese to morbidly obese children are also more likely to begin puberty earlier than children of normal weight.[11] Variation in genes related to obesity such as FTO or NEGRI have been associated with earlier onset of puberty.[7] Children whose parents started puberty at an earlier age were also more likely to experience it themselves, especially in women where onset of menstruation correlated well between mothers and daughters and between sisters.[7]
Constitutional delay
Children with constitutional delay report that they are shorter than their peer, that their growth has slowed down, and that they are thinner than their classmates.[12] Their growth has begun to slow down years before the expected growth spurt secondary to puberty, which helps differentiate a constitutional delay from an HPG-axis related disorder.[10] A complete family history with the ages at which parents hit the puberty milestones can also provide a reference point for the expected age of puberty.[4][7] Growth measurement parameters in children with suspected constitutional delay include a height, a weight, the rate of growth, and the calculated mid-parental height which represents the expected adult height for the child.[3][4]
Chronic disease
Diet and physical activity habits, as well as history of previous serious illnesses and medication history can provide clues as to the cause of delayed puberty.[7] Delayed growth and puberty can be the first signs of severe chronic illnesses such as metabolic disorders including inflammatory bowel disease and hypothyroidism.[7] Symptoms such as fatigue, pain, and abnormal stooling pattern are suggestive of an underlying chronic condition.[4] Low BMI can lead a physician to diagnose an eating disorder, undernutrition, child abuse, or chronic gastrointestinal disorders.[4]
Primary gonad failure
A eunuchoid body shape where the arm span exceeds the height by more than 5 cm suggests a delay in growth plate closure secondary to hypogonadism.[7] Turner syndrome has unique diagnostic features including a webbed neck, short stature, shield chest, and low hairline.[4] Klinefelter syndrome presents with tall stature as well as small, firm testes.[4]
Hormonal pathway defects
Lacking the sense of smell (anosmia) along with delayed puberty are strong clinical indications for Kallmann syndrome.[10][13][14] Deficiencies in GnRH, the signalling hormone produced by the hypothalamus, can cause congenital malformations including cleft lip and scoliosis.[7] The presence of neurological symptoms including headaches and visual disturbances suggest a brain disorder such as a brain tumor causing hypopituitarism.[7] The presence of neurological symptoms in addition to lactation are signs of high prolactin levels and could indicate either a drug side effect or a prolactinoma.[4]
Causes
Pubertal delay can be separated into four categories from most to least common:[3]
Constitutional delay
Children who are healthy but have a slower rate of physical development than average have a constitutional delay with a subsequent delay in puberty. It is the most common cause of delayed puberty in girls[15][8] (30%)[7] and even more so in boys[3] (65%).[10] It is commonly inherited with as much as 80% of the variation in the age of onset of puberty due to genetic factors.[10][16] These children have a history of shorter stature than their age-matched peers throughout childhood, but their height is appropriate for bone age, meaning that they have delayed skeletal maturation with potential for future growth.[7]
It is often difficult to establish if it is a true constitutional delay of growth and puberty or if there is an underlying pathology because lab tests are not always discriminatory.[17] In absence of any other symptoms, short stature, delayed growth in height and weight, and/or delayed puberty may be the only clinical manifestations of certain chronic diseases including coeliac disease.[18][19][20][21]
Chronic disease
When underweight or sickly children present with pubertal delay, it is warranted to search for illnesses that cause a temporary and reversible delay in puberty.[3] Chronic conditions such as sickle cell disease[22][23][24] and thalassemia,[25] cystic fibrosis,[26] HIV/AIDS, hypothyroidism,[27] chronic kidney disease,[28][29] and chronic gastroenteric disorders (such as coeliac disease[19][30] and inflammatory bowel disease[31][32][33]) cause a delayed activation of the hypothalamic region of the brain to send signals to start puberty.[34]
Childhood cancer survivors can also present with delayed puberty secondary to their cancer treatments, especially males.[10][12] The type of treatment, amount of exposure/dosage of drugs, and age during treatment determine the level by which the gonads are affected with younger patients at a lower risk of negative reproductive effects.[12]
Excessive physical exercise and physical stress, especially in athletes can also delay pubertal onset.[35] Eating disorders such as bulimia nervosa and anorexia nervosa can also impair puberty due to undernutrition.[34][36]
Carbohydrate-restricted diets for weight loss has also been shown to decrease the stimulation of insulin which in turn does not stimulate kisspeptin neurons vital in the release of puberty-starting hormones.[37] This shows that carbohydrate restricted children and children with diabetes mellitus type 1 can have delayed puberty.[11][38]
Primary gonad failure
Primary failure of the ovaries or testes (gonads) (hypergonadotropic hypogonadism) will cause delayed puberty due to the lack of hormonal response by the final receptors of the HPG axis.[7] In this scenario, the brain sends a lot of hormonal signals (high gonadotropin), but the gonads are unable to respond to said signals causing hypergonadotropic hypogonadism.[7] Hypergonadotropic hypogonadism can be caused by congenital defects or acquired defects.[39]
Congenital disorders
Congenital diseases include untreated cryptorchidism where the testicles fail to descend from the abdomen.[34] Other congenital disorders are genetic in nature. In males, there can be deformities in the seminiferous tubule as in Klinefelter syndrome (most common cause in males),[40] defects in the production of testicular steroids, receptor mutations preventing testicular hormones from working, chromosomal abnormalities such as Noonan syndrome, or problems with the cells making up the testes.[34] Females can also have chromosomal abnormalities such as Turner syndrome (most common cause in girls),[40] XX gonadal dysgenesis, and XY gonadal dysgenesis, problems in the ovarian hormone synthesis pathway such as aromatase deficiency[34] or congenital anatomical deformities such as Müllerian agenesis.[39]
Acquired disorders
Acquired diseases include mumps orchitis, Coxsackievirus B infection, irradiation, chemotherapy, or trauma; all problems causing the gonads to fail.[3][39]
Hormonal pathway defects
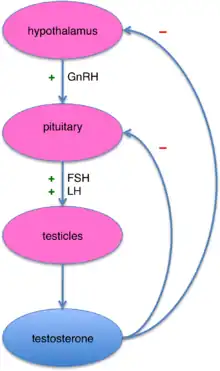
The hypothalamic–pituitary–gonadal axis can also be affected at the level of the brain.[39] The brain does not send its hormonal signals to the gonads (low gonadotropins) causing the gonads to never be activated in the first place resulting in hypogonadotropic hypogonadism.[41] The HPG axis can be altered in two places, at the hypothalamic or at the pituitary level.[41] CNS disorders such as childhood brain tumors (e.g. craniopharyngioma, prolactinoma, germinoma, glioma) can disrupt the communication between the hypothalamus and the pituitary.[34] Pituitary tumors, especially prolactinomas, can increase the level of dopamine causing an inhibiting effect to the HPG axis.[15] Hypothalamic disorders include Prader-Willi syndrome and Kallmann syndrome,[3] but the most common cause of hypogonadotropic hypogonadism is a functional deficiency in the hormone regulator produced by the hypothalamus, the gonadotropin-releasing hormone or GnRH.[7]
Diagnosis
A complete medical history, review of systems, growth pattern, and physical examination as well as laboratory testing and imaging will reveal most of the systemic diseases and conditions capable of arresting development or delaying puberty, as well as providing clues to some of the recognizable syndromes affecting the reproductive system.[7]
Timely medical assessment is a necessity since as many as half of girls with delayed puberty have an underlying pathology.[8]
Lab tests
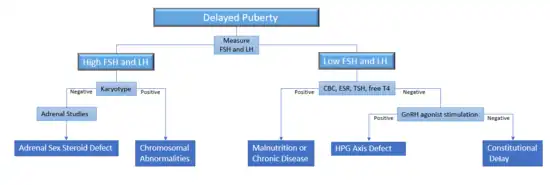
The first step in evaluating children with delayed puberty involves differentiating between the different causes of delayed puberty. Constitutional delay can be evaluated with a thorough history, physical, and bone age.[4] Malnutrition and chronic diseases can be diagnosed through history and disease-specific testing.[3] Screening studies include a complete blood count, an erythrocyte sedimentation rate, and thyroid studies[3]. Hypogonadism can be differentiated between hyper- and hypo-gonadotropic hypogonadism by measuring serum follicle-stimulating hormone (FSH) and luteinizing hormone (LH) (gonadotropins to measure pituitary output), and estradiol in girls (to measure gonadal output).[7][39] By the age of 10-12, children with failure of the ovaries or testes will have high LH and FSH because the brain is attempting to jump-start puberty, but the gonads are not responsive to these signals.[7][3]
Stimulating the body by administering an artificial version of gonadotropin-releasing hormone (GnRH, the hypothalamic hormone) can differentiate between constitutional delay of puberty and a GnRH deficiency in boys, although no studies have been done in girls to prove this.[7][42] It is often sufficient to simply measure the baseline gonadotrophin levels to differentiate between the two.[10]
In girls with hypogonadotropic hypogonadism, a serum prolactin level is measured to identify if they have the pituitary tumor prolactinoma. High levels of prolactin would warrant further testing with MRI imaging, except if drugs inducing the production of prolactin can be identified.[7] If the child has any neurological symptoms, it is highly recommended that the physician obtains a head MRI to detect possible brain lesions.[7]
In girls with hypergonadotropic hypogonadism, a karyotype can identify chromosomal abnormalities, the most common of which is Turner syndrome.[7] In boys, a karyotype is indicated if the child may have a congenital gonadal defect such as Klinefelter syndrome.[3] In children with a normal karyotype, defects in the synthesis of the adrenal steroid sex hormones can be identified by measuring 17-hydroxylase, an important enzyme involved in the production of sex hormones.[7]
Imaging

Since bone maturation is a good indicator of overall physical maturation, an x-ray of the left hand and wrist to assess bone age usually reveals whether the child has reached a stage of physical maturation at which puberty should be occurring.[3][7] X-ray displaying a bone age <11 years in girls or <13 years in boys (despite a higher chronological age) is most often consistent with constitutional delay of puberty.[7][40] An MRI of the brain should be considered if neurological symptoms are present in addition to delayed puberty, two findings suspicious for pituitary or hypothalamic tumors.[3][10] An MRI can also confirm the diagnosis of Kallmann syndrome due to the absence or abnormal development of the olfactory tract.[10] However in the absence of clear neurological symptoms, an MRI may not be the most cost-effective option.[10] A pelvic ultrasound can detect anatomical abnormalities including undescended testes and müllerian agenesis.[3][39]
Management
The goals of short-term hormone therapy are to induce the beginning of sexual development and induce a growth spurt, but should be limited to children with severe distress or anxiety secondary to their delayed puberty.[3][7] Bone age must be monitored frequently to prevent precocious closure of the bone plates, thereby stunting growth.[7]
Constitutional delay
If a child is healthy with a constitutional delay of growth and puberty, reassurance and prediction based on the bone age can be provided.[10][12] No other intervention is usually necessary, but repeat evaluation by measuring serum testosterone or estrogen is recommended.[3][4][7] Furthermore, the diagnosis of hypogonadism can be excluded once the adolescent has started puberty by age 16-18.[4][40]
Boys aged >14 years old whose growth is severely stunted or are experiencing severe distress secondary to their lack of puberty can be started on testosterone to increase their height.[10] Testosterone treatment can also be used to stimulate sexual development, but it can close bone plates prematurely stopping growth altogether if not carefully administered.[43][7] Another therapeutic option is the use of aromatase inhibitors to inhibit the conversion of androgens to estrogens as estrogens are responsible for stopping bone growth plate development and thus growth.[10] However, due to side effects, therapy with testosterone alone is most often used.[10] Overall, neither growth hormone nor aromatase inhibitors are recommended for constitutional delay to increase growth.[12][44]
Girls can be started on estrogen with the same goals as their male counterparts.[10]
Overall, studies have shown no significant difference in final adult height between adolescents treated with sex steroids and those who were only observed with no treatment.[45]
Chronic disease
If the delay is due to systemic disease or malnutrition, the therapeutic intervention is likely to focus direction on those conditions. In patients with coeliac disease, an early diagnosis and the establishment of a gluten-free diet prevents long-term complications and allows restoration of normal maturation.[18][21] Thyroid hormone therapy will be necessary in the case of hypothyroidism.[7]
Primary gonad failure
Whereas children with constitutional delay will have normal levels of sex hormones post-puberty, gonadotropin deficiency or hypogonadism may require lifelong sex steroid replacement.[3]
In girls with primary ovarian failure, estrogen should be started when puberty is supposed to start.[7] Progestins are usually added after there is acceptable breast development, about 12 to 24 months after starting estrogen, as starting treatment with progestin too early can negatively affect breast growth.[7] After acceptable breast growth, administering estrogen and progestin in a cyclical manner can help establish regular menses once puberty is started.[43][40] The goal is to complete sexual maturation over 2 to 3 years.[7] Once sexual maturation has been achieved, a trial period with no hormonal therapy can determine whether or not the child will require life-long treatment.[3] Girls with congenital GnRH deficiency require enough sex hormone supplementation to maintain body levels in the expected pubertal levels necessary to induce ovulation, especially when fertility is a concern.[7]
Males with primary failure of the testes will be on lifelong testosterone.[14]
Pulsatile GnRH, weekly multi-LH, or hCG and FSH can be used to induce fertility in adulthood for both males and females.[10][40]
Hormonal pathway defects
Boys aged >12 years old with hypogonadotropic hypogonadism are most often treated with short-term testosterone while males with testicular failure will be on life-long testosterone.[10][46][47] Choice of formulation (topical vs injection) is dependent on the child's and family's preference as well as on how well they tolerate side effects.[46] Although testosterone therapy alone will result in the start of puberty, to increase fertility potential, they may need pulsatile GnRH or hCG with rFSH.[10][46] hCG can be used by itself in boys with spontaneous onset of puberty from non-permanent forms of hypogonadotropic hypogonadism and rFSH can be added in cases of low sperm count after 6 to 12 months of treatment.[10]
If puberty has not started after 1 year of treatment, then permanent hypogonadotropic hypogonadism should be considered.[10]
Girls with hypogonadotropic hypogonadism are started on the same sex steroid therapy as their counterparts with a constitutional delay, however doses are gradually increased to reach full adult replacement levels.[10] Dosage of estrogen is titrated based on the woman's ability to have withdrawal bleeds and to maintain appropriate bone density.[10] Induction of fertility must also be done through pulsatile GnRH.[10]
Others
Growth hormone is another option that has been described, however it should only be used in proven growth hormone deficiency[48][49] such as idiopathic short stature.[10] Children with a constitutional delay have not been shown to benefit from growth hormone therapy.[10] Although serum growth hormone levels are low in constitutional delay of puberty, they increase after treatment with sex hormones and in those cases, growth hormone is not suggested to accelerate growth.[7]
Subnormal vitamin A intake is one of the etiological factors in delayed pubertal maturation. Supplementation of both vitamin A and iron to normal constitutionally delayed children with subnormal vitamin A intake is as efficacious as hormonal therapy in the induction of growth and puberty.[50]
More therapies are being developed to target the more discreet modulators of the HPG axis including kisspeptin and neurokinin B.[51][52]
In cases of severe delayed puberty secondary to hypogonadism, evaluation by a psychologist or psychiatrist, as well as counseling and a supportive environment are an important supplemental therapy for the child.[3][53] Transition from pediatric to adult care is also vital as many children are lost during transition of care.[12]
Outcomes
Constitutional delay of growth and puberty is a variation of normal development with no long-term health consequences, however it can have lasting psychological effects.[45][54] Adolescent boys with delayed puberty have a higher level of anxiety and depression relative to their peers.[55] Children with delayed puberty also display decreased academic performance in their adolescent education, but changes in academic achievement in adulthood have not been determined.[45]
There is conflicting evidence as to whether or not children with constitutional growth and pubertal delay reach their full height potential.[45] The conventional teaching is that these children catch up on their growth during the pubertal growth spurt and just remain shorter before their delayed puberty starts.[56] However, some studies show that these children fall short of their target height from about 4 to 11 cm.[45] Factors that could affect final height include familial short stature and pre-pubertal growth development.[45]
Pubertal delay can also affect bone mass and subsequent development of osteoporosis.[57] Men with delayed puberty often have low to normal bone mineral density unaffected by androgen therapy.[45] Women are more likely to have lower bone mineral density and thus an increased risk of fractures as early as even before the onset of puberty.[45]
Furthermore delayed puberty is correlated with a higher risk in cardiovascular and metabolic disorders in women only, but also appears to be protective for breast and endometrial in women and testicular cancer in men.[45]
References
- 1 2 3 4 5 6 7 Tang, C; Zafar Gondal, A; Damian, M (January 2020). "Delayed Puberty". PMID 31335042.
{{cite journal}}: Cite journal requires|journal=(help) - 1 2 3 4 Howard SR, Dunkel L (2018). "The Genetic Basis of Delayed Puberty". Neuroendocrinology. 106 (3): 283–291. doi:10.1159/000481569. PMID 28926843.
- 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 Ferri, Fred F. (2018). Ferri's Clinical Advisor 2019 E-Book: 5 Books in 1. Elsevier Health Sciences. p. 412.e3. ISBN 978-0-323-55076-5. Archived from the original on 24 June 2021. Retrieved 21 February 2021.
- 1 2 3 4 5 6 7 8 9 10 11 12 13 14 Klein DA, Emerick JE, Sylvester JE, Vogt KS (November 2017). "Disorders of Puberty: An Approach to Diagnosis and Management". American Family Physician. 96 (9): 590–599. PMID 29094880.
- ↑ Schultz, James Alfred (2015). The Knowledge of Childhood in the German Middle Ages, 1100-1350. University of Pennsylvania Press. p. 11. ISBN 978-1-5128-0667-0. Archived from the original on 2021-06-24. Retrieved 2021-02-21.
- ↑ Lewis, Mary (12 February 2018). "Children aren't starting puberty younger, medieval skeletons reveal". The Conversation. Archived from the original on 17 January 2021. Retrieved 21 February 2021.
- 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 Fritz, Marc A; Speroff, Leon (2015). Clinical Gynecologic Endocrinology and Infertility. Lippincott Williams & Wilkins. ISBN 9781451189766. OCLC 885230917.
- 1 2 3 4 5 6 7 8 Adams, Paula J. Hillard (2013). Practical pediatric and adolescent gynecology. Wiley-Blackwell. ISBN 9781118538586. OCLC 929718561.
- ↑ Traggiai C, Stanhope R (February 2003). "Disorders of pubertal development". Best Practice & Research. Clinical Obstetrics & Gynaecology. 17 (1): 41–56. doi:10.1053/ybeog.2003.0360. PMID 12758225.
- 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 Dunkel L, Quinton R (June 2014). "Transition in endocrinology: induction of puberty". European Journal of Endocrinology. 170 (6): R229–39. doi:10.1530/EJE-13-0894. PMID 24836550.
- 1 2 Richmond HM, Duriancik DM (September 2017). "Impact of Carbohydrate Restriction on Healthy Adolescent Development". Pediatric Endocrinology Reviews. 15 (1): 26–32. doi:10.17458/per.vol15.2017.rd.impactcarbohydraterestriction. PMID 28845625.
- 1 2 3 4 5 6 Dwyer AA, Phan-Hug F, Hauschild M, Elowe-Gruau E, Pitteloud N (July 2015). "TRANSITION IN ENDOCRINOLOGY: Hypogonadism in adolescence". European Journal of Endocrinology. 173 (1): R15–24. doi:10.1530/EJE-14-0947. PMID 25653257.
- ↑ Oxford Endocrinology Library. Testosterone Deficiency in Men. 2008. ISBN 978-0199545131 Editor: Hugh Jones. Chapter 9. Puberty & Fertility.
- 1 2 Male Hypogonadism. Friedrich Jockenhovel. Uni-Med Science. 2004. ISBN 3-89599-748-X. Chapter 3. Diagnostic work up of hypogonadism.
- 1 2 Hoffman, Barbara (2016). Williams Gynecology. McGraw-Hill Education. ISBN 978-0-07-184908-1.
- ↑ Howard SR, Dunkel L (August 2018). "Management of hypogonadism from birth to adolescence". Best Practice & Research. Clinical Endocrinology & Metabolism. Issue Update in paediatric endocrinology. 32 (4): 355–372. doi:10.1016/j.beem.2018.05.011. PMID 30086863. Archived from the original on 2020-01-28. Retrieved 2019-12-13.
- ↑ Wei C, Crowne EC (May 2016). "Recent advances in the understanding and management of delayed puberty". Archives of Disease in Childhood (Review). 101 (5): 481–8. doi:10.1136/archdischild-2014-307963. PMID 26353794.
- 1 2 Mearin ML (June 2015). "The prevention of coeliac disease". Best Practice & Research. Clinical Gastroenterology (Review). 29 (3): 493–501. doi:10.1016/j.bpg.2015.04.003. PMID 26060113.
- 1 2 Leffler DA, Green PH, Fasano A (October 2015). "Extraintestinal manifestations of coeliac disease". Nature Reviews. Gastroenterology & Hepatology (Review). 12 (10): 561–71. doi:10.1038/nrgastro.2015.131. PMID 26260366.
- ↑ Guandalini S, Assiri A (March 2014). "Celiac disease: a review". JAMA Pediatrics. 168 (3): 272–8. doi:10.1001/jamapediatrics.2013.3858. PMID 24395055.
- 1 2 Levy J, Bernstein L, Silber N (December 2014). "Celiac disease: an immune dysregulation syndrome". Current Problems in Pediatric and Adolescent Health Care (Review). 44 (11): 324–7. doi:10.1016/j.cppeds.2014.10.002. PMID 25499458.
- ↑ Aeddula, Narothama Reddy; Baradhi, Krishna M. (2018), "Sickle Cell Nephropathy", StatPearls, StatPearls Publishing, PMID 30252273, archived from the original on 2021-08-28, retrieved 2019-01-26
- ↑ Stimpson SJ, Rebele EC, DeBaun MR (2016). "Common gynecological challenges in adolescents with sickle cell disease". Expert Review of Hematology. 9 (2): 187–96. doi:10.1586/17474086.2016.1126177. PMID 26613137.
- ↑ Huang AW, Muneyyirci-Delale O (July 2017). "Reproductive endocrine issues in men with sickle cell anemia". Andrology. 5 (4): 679–690. doi:10.1111/andr.12370. PMID 28662541.
- ↑ Castaldi MA, Cobellis L (June 2016). "Thalassemia and infertility". Human Fertility. 19 (2): 90–6. doi:10.1080/14647273.2016.1190869. PMID 27335221.
- ↑ Johannesson M, Gottlieb C, Hjelte L (January 1997). "Delayed puberty in girls with cystic fibrosis despite good clinical status". Pediatrics. 99 (1): 29–34. doi:10.1542/peds.99.1.29. PMID 8989333.
- ↑ Tsutsui K, Son YL, Kiyohara M, Miyata I (January 2018). "Discovery of GnIH and Its Role in Hypothyroidism-Induced Delayed Puberty". Endocrinology. 159 (1): 62–68. doi:10.1210/en.2017-00300. PMID 28938445.
- ↑ Thébaut A, Amouyal M, Besançon A, Collet M, Selbonne E, Valentin C, Vonthron M, Zakariya M, Linglart A (June 2013). "[Puberty, fertility and chronic diseases]". Archives de Pediatrie (Review). 20 (6): 673–84. doi:10.1016/j.arcped.2013.03.015. PMID 23619213.
- ↑ Haffner D, Zivicnjak M (June 2017). "Pubertal development in children with chronic kidney disease". Pediatric Nephrology. 32 (6): 949–964. doi:10.1007/s00467-016-3432-3. PMID 27464647.
- ↑ Tersigni C, Castellani R, de Waure C, Fattorossi A, De Spirito M, Gasbarrini A, Scambia G, Di Simone N (2014). "Celiac disease and reproductive disorders: meta-analysis of epidemiologic associations and potential pathogenic mechanisms". Human Reproduction Update (Review). 20 (4): 582–93. doi:10.1093/humupd/dmu007. PMID 24619876.
- ↑ Sanderson IR (October 2014). "Growth problems in children with IBD". Nature Reviews. Gastroenterology & Hepatology (Review). 11 (10): 601–10. doi:10.1038/nrgastro.2014.102. PMID 24957008.
- ↑ Wong SC, Catto-Smith AG, Zacharin M (February 2014). "Pathological fractures in paediatric patients with inflammatory bowel disease". European Journal of Pediatrics (Review). 173 (2): 141–51. doi:10.1007/s00431-013-2174-5. PMID 24132387.
- ↑ Corica D, Romano C (February 2017). "Biological Therapy in Pediatric Inflammatory Bowel Disease: A Systematic Review". Journal of Clinical Gastroenterology. 51 (2): 100–110. doi:10.1097/MCG.0000000000000696. PMID 27636407.
- 1 2 3 4 5 6 Schlomo, Melmed (2015). Williams textbook of endocrinology. Elsevier. ISBN 978-0323341578. OCLC 995483654.
- ↑ Maïmoun L, Georgopoulos NA, Sultan C (November 2014). "Endocrine disorders in adolescent and young female athletes: impact on growth, menstrual cycles, and bone mass acquisition". The Journal of Clinical Endocrinology and Metabolism (Review). 99 (11): 4037–50. doi:10.1210/jc.2013-3030. PMID 24601725.
- ↑ Kapczuk K (October 2017). "Elite athletes and pubertal delay". Minerva Pediatrica. 69 (5): 415–426. doi:10.23736/S0026-4946.17.05044-7. PMID 28745464.
- ↑ Pankov YA (September 2015). "[Kisspeptin and leptin in the regulation of fertility]". Molekuliarnaia Biologiia. 49 (5): 707–15. doi:10.7868/S0026898415050134. PMID 26510589.
- ↑ Gandhi J, Dagur G, Warren K, Smith NL, Sheynkin YR, Zumbo A, Khan SA (2017). "The Role of Diabetes Mellitus in Sexual and Reproductive Health: An Overview of Pathogenesis, Evaluation, and Management". Current Diabetes Reviews. 13 (6): 573–581. doi:10.2174/1573399813666161122124017. PMID 27875946.
- 1 2 3 4 5 6 Goldman, Lee (2015). Goldman-Cecil Medicine. Elsevier. ISBN 978-1455750177.
- 1 2 3 4 5 6 Villanueva C, Argente J (2014). "Pathology or normal variant: what constitutes a delay in puberty?". Hormone Research in Paediatrics. 82 (4): 213–21. doi:10.1159/000362600. PMID 25011467.
- 1 2 Pariseai M (2008). "Gynaecological endocrinology". Obstetrics and gynaecology. St. Louis: Mosby. ISBN 9780723434726.
- ↑ Jungmann E, Trautermann C (October 1994). "[The status of the gonadotropin releasing hormone test in differential diagnosis of delayed puberty in adolescents over 14 years of age]". Medizinische Klinik (in German). 89 (10): 529–33. PMID 7808353.
{{cite journal}}: CS1 maint: unrecognized language (link) - 1 2 Wecker, Lynn (2010). Brody's human pharmacology : molecular to clinical. Elsevier Mosby. ISBN 9780323053747. OCLC 804133604.
- ↑ Wit JM, Oostdijk W (June 2015). "Novel approaches to short stature therapy". Best Practice & Research. Clinical Endocrinology & Metabolism. Hormone replacement strategies in paediatric and adolescent endocrine disorders. 29 (3): 353–66. doi:10.1016/j.beem.2015.01.003. PMID 26051296.
- 1 2 3 4 5 6 7 8 9 Zhu J, Chan YM (June 2017). "Adult Consequences of Self-Limited Delayed Puberty". Pediatrics. 139 (6): e20163177. doi:10.1542/peds.2016-3177. PMID 28562264.
- 1 2 3 Watson S, Fuqua JS, Lee PA (February 2014). "Treatment of hypogonadism in males". Pediatric Endocrinology Reviews. 11 Suppl 2: 230–9. PMID 24683947.
- ↑ Legato MJ, Bilezikian JP (2004). Legato MJ (ed.). Principles of Gender-Specific Medicine. Vol. 1–2. p. 22. ISBN 978-0-12-440905-7.
- ↑ Heinrichs C, Bourguignon JP (1991). "Treatment of delayed puberty and hypogonadism in girls". Hormone Research. 36 (3–4): 147–52. doi:10.1159/000182149. PMID 1818011.
- ↑ Massa G, Heinrichs C, Verlinde S, Thomas M, Bourguignon JP, Craen M, François I, Du Caju M, Maes M, De Schepper J (September 2003). "Late or delayed induced or spontaneous puberty in girls with Turner syndrome treated with growth hormone does not affect final height". The Journal of Clinical Endocrinology and Metabolism. 88 (9): 4168–74. doi:10.1210/jc.2002-022040. PMID 12970282.
- ↑ Zadik Z, Sinai T, Zung A, Reifen R (June 2004). "Vitamin A and iron supplementation is as efficient as hormonal therapy in constitutionally delayed children". Clinical Endocrinology. 60 (6): 682–7. doi:10.1111/j.1365-2265.2004.02034.x. PMID 15163330.
- ↑ Newton CL, Anderson RC, Millar RP (2016). Therapeutic Neuroendocrine Agonist and Antagonist Analogs of Hypothalamic Neuropeptides as Modulators of the Hypothalamic-Pituitary-Gonadal Axis. Endocrine Development. Vol. 30. pp. 106–29. doi:10.1159/000439337. ISBN 978-3-318-05636-5. PMID 26684214.
- ↑ Wei C, Crowne EC (May 2016). "Recent advances in the understanding and management of delayed puberty". Archives of Disease in Childhood. 101 (5): 481–8. doi:10.1136/archdischild-2014-307963. PMID 26353794.
- ↑ Berenbaum SA, Beltz AM, Corley R (2015). The importance of puberty for adolescent development: conceptualization and measurement. Advances in Child Development and Behavior. Vol. 48. pp. 53–92. doi:10.1016/bs.acdb.2014.11.002. ISBN 9780128021781. PMID 25735941.
- ↑ Jameson, J. Larry; de Kretser, David; Marshall, John C. (2013). Endocrinology adult and pediatric : reproductive endocrinology (6th ed.). Philadelphia. ISBN 9780323240604. OCLC 881479176.
- ↑ Dwyer AA, Phan-Hug F, Hauschild M, Elowe-Gruau E, Pitteloud N (July 2015). "TRANSITION IN ENDOCRINOLOGY: Hypogonadism in adolescence". European Journal of Endocrinology. 173 (1): R15–24. doi:10.1530/EJE-14-0947. PMID 25653257.
- ↑ Prader A (March 1975). "Delayed adolescence". Clinics in Endocrinology and Metabolism. 4 (1): 143–55. doi:10.1016/S0300-595X(75)80037-5. PMID 166776.
- ↑ NIH Consensus Development Panel on Osteoporosis Prevention Diagnosis and Therapy (February 2001). "Osteoporosis prevention, diagnosis, and therapy". JAMA. 285 (6): 785–95. doi:10.1001/jama.285.6.785. PMID 11176917.
External links
| Classification |
|---|