Epilepsy
| Epilepsy | |
|---|---|
| Other names: Seizure disorder | |
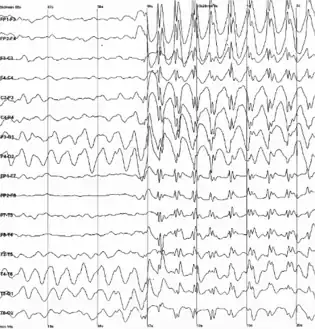 | |
| Generalized 3 Hz spike-and-wave discharges on an electroencephalogram | |
| Specialty | Neurology |
| Symptoms | Periods of vigorous shaking, nearly undetectable spells[1] |
| Duration | Long term[2] |
| Causes | Unknown, brain injury, stroke, brain tumors, infections of the brain, birth defects[2][3][4] |
| Diagnostic method | Electroencephalogram, ruling out other possible causes[5] |
| Differential diagnosis | Fainting, alcohol withdrawal, electrolyte problems[5] |
| Treatment | Medication, surgery, neurostimulation, dietary changes[6][7] |
| Prognosis | Controllable in 70%[8] |
| Frequency | 50 million (2022)[1] |
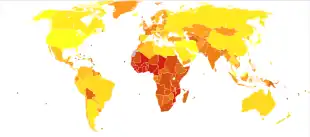
| Deaths | 125,000 (2015)[9] |
Epilepsy is a group of neurological disorders characterized by recurrent epileptic seizures.[10] Epileptic seizures are episodes that can vary from brief and nearly undetectable periods to long periods of vigorous shaking.[1] These episodes can result in physical injuries, including occasionally broken bones.[2] In epilepsy, seizures have a tendency to recur and, as a rule, have no immediate underlying cause.[11] Isolated seizures that are provoked by a specific cause such as poisoning are not deemed to represent epilepsy.[12] People with epilepsy may be treated differently in various areas of the world and experience varying degrees of social stigma due to their condition.[2]
The underlying mechanism of epileptic seizures is excessive and abnormal neuronal activity in the cortex of the brain.[12] The reason this occurs in most cases of epilepsy is unknown.[2] Some cases occur as the result of brain injury, stroke, brain tumors, infections of the brain, or birth defects through a process known as epileptogenesis.[2][3][4] Known genetic mutations are directly linked to a small proportion of cases.[5][13] The diagnosis involves ruling out other conditions that might cause similar symptoms, such as fainting, and determining if another cause of seizures is present, such as alcohol withdrawal or electrolyte problems.[5] This may be partly done by imaging the brain and performing blood tests.[5] Epilepsy can often be confirmed with an electroencephalogram (EEG), but a normal test does not rule out the condition.[5]
Epilepsy that occurs as a result of other issues may be preventable.[2] Seizures are controllable with medication in about 70% of cases;[8] inexpensive anti-seizure medications are often available.[2] In those whose seizures do not respond to medication, surgery, neurostimulation or dietary changes may then be considered.[6][7] Not all cases of epilepsy are lifelong, and many people improve to the point that treatment is no longer needed.[2]
As of 2022, about 50 million people have epilepsy (0.5-1% of the population).[14][1] Around 70% of cases occur in the developing world.[1] In 2015, it resulted in 125,000 deaths, an increase from 112,000 in 1990.[9][15] Epilepsy is more common in older people.[16][17] In the developed world, onset of new cases occurs most frequently in babies and the elderly.[18] In the developing world, onset is more common in older children and young adults due to differences in the frequency of the underlying causes.[19] About 5–10% of people will have an unprovoked seizure by the age of 80,[20] and the chance of experiencing a second seizure is between 40 and 50%.[21] In many areas of the world, those with epilepsy either have restrictions placed on their ability to drive or are not permitted to drive until they are free of seizures for a specific length of time.[22] The word epilepsy is from Ancient Greek ἐπιλαμβάνειν, 'to seize, possess, or afflict'.[23]
Signs and symptoms
Epilepsy is characterized by a long-term risk of recurrent seizures.[24] These seizures may present in several ways depending on the part of the brain involved and the person's age.[24][25]
Seizures
The most common type (60%) of seizures are convulsive.[25] Of these, one-third begin as generalized seizures from the start, affecting both hemispheres of the brain.[25] Two-thirds begin as focal seizures (which affect one hemisphere of the brain) which may then progress to generalized seizures.[25] The remaining 40% of seizures are non-convulsive. An example of this type is the absence seizure, which presents as a decreased level of consciousness and usually lasts about 10 seconds.[3][26]
Focal seizures are often preceded by certain experiences, known as auras.[27] They include sensory (visual, hearing, or smell), psychic, autonomic, and motor phenomena.[3] Jerking activity may start in a specific muscle group and spread to surrounding muscle groups in which case it is known as a Jacksonian march.[28] Automatisms may occur, which are non-consciously-generated activities and mostly simple repetitive movements like smacking of the lips or more complex activities such as attempts to pick up something.[28]
There are six main types of generalized seizures: tonic-clonic, tonic, clonic, myoclonic, absence and atonic seizures.[29] They all involve loss of consciousness and typically happen without warning.
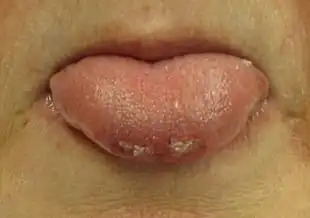
Tonic-clonic seizures occur with a contraction of the limbs followed by their extension along with arching of the back which lasts 10–30 seconds (the tonic phase). A cry may be heard due to contraction of the chest muscles, followed by a shaking of the limbs in unison (clonic phase). Tonic seizures produce constant contractions of the muscles. A person often turns blue as breathing is stopped. In clonic seizures there is shaking of the limbs in unison. After the shaking has stopped it may take 10–30 minutes for the person to return to normal; this period is called the "postictal state" or "postictal phase." Loss of bowel or bladder control may occur during a seizure.[30] The tongue may be bitten at either the tip or on the sides during a seizure.[31] In tonic-clonic seizure, bites to the sides are more common.[31] Tongue bites are also relatively common in psychogenic non-epileptic seizures.[31]
Myoclonic seizures involve spasms of muscles in either a few areas or all over.[32] Absence seizures can be subtle with only a slight turn of the head or eye blinking.[3] The person does not fall over and returns to normal right after it ends.[3] Atonic seizures involve the loss of muscle activity for greater than one second.[28] This typically occurs on both sides of the body.[28]
About 6% of those with epilepsy have seizures that are often triggered by specific events and are known as reflex seizures.[33] Those with reflex epilepsy have seizures that are only triggered by specific stimuli.[34] Common triggers include flashing lights and sudden noises.[33] In certain types of epilepsy, seizures happen more often during sleep,[35] and in other types they occur almost only when sleeping.[36]
Post-ictal
After the active portion of a seizure (the ictal state) there is typically a period of recovery during which there is confusion, referred to as the postictal period before a normal level of consciousness returns.[27] It usually lasts 3 to 15 minutes[37] but may last for hours.[38] Other common symptoms include feeling tired, headache, difficulty speaking, and abnormal behavior.[38] Psychosis after a seizure is relatively common, occurring in 6–10% of people.[39] Often people do not remember what happened during this time.[38] Localized weakness, known as Todd's paralysis, may also occur after a focal seizure. When it occurs it typically lasts for seconds to minutes but may rarely last for a day or two.[40]
Psychosocial
Epilepsy can have adverse effects on social and psychological well-being.[25] These effects may include social isolation, stigmatization, or disability.[25] They may result in lower educational achievement and worse employment outcomes.[25] Learning disabilities are common in those with the condition, and especially among children with epilepsy.[25] The stigma of epilepsy can also affect the families of those with the disorder.[30]
Certain disorders occur more often in people with epilepsy, depending partly on the epilepsy syndrome present. These include depression, anxiety, obsessive–compulsive disorder (OCD),[41] and migraine.[42] Attention deficit hyperactivity disorder affects three to five times more children with epilepsy than children without the condition.[43] ADHD and epilepsy have significant consequences on a child's behavioral, learning, and social development.[44] Epilepsy is also more common in children with autism.[45]
Causes
Epilepsy can have both genetic and acquired causes, with interaction of these factors in many cases.[46] Established acquired causes include serious brain trauma, stroke, tumours and problems in the brain as a result of a previous infection.[46] In about 60% of cases the cause is unknown.[25][30] Epilepsies caused by genetic, congenital, or developmental conditions are more common among younger people, while brain tumors and strokes are more likely in older people.[25]
Seizures may also occur as a consequence of other health problems;[29] if they occur right around a specific cause, such as a stroke, head injury, toxic ingestion or metabolic problem, they are known as acute symptomatic seizures and are in the broader classification of seizure-related disorders rather than epilepsy itself.[47][48]
Genetics
Genetics is believed to be involved in the majority of cases, either directly or indirectly.[13] Some epilepsies are due to a single gene defect (1–2%); most are due to the interaction of multiple genes and environmental factors.[13] Each of the single gene defects is rare, with more than 200 in all described.[49] Most genes involved affect ion channels, either directly or indirectly.[46] These include genes for ion channels themselves, enzymes, GABA, and G protein-coupled receptors.[32]
In identical twins, if one is affected there is a 50–60% chance that the other will also be affected.[13] In non-identical twins the risk is 15%.[13] These risks are greater in those with generalized rather than focal seizures.[13] If both twins are affected, most of the time they have the same epileptic syndrome (70–90%).[13] Other close relatives of a person with epilepsy have a risk five times that of the general population.[50] Between 1 and 10% of those with Down syndrome and 90% of those with Angelman syndrome have epilepsy.[50]
Acquired
Epilepsy may occur as a result of a number of other conditions including tumors, strokes, head trauma, previous infections of the central nervous system, genetic abnormalities, and as a result of brain damage around the time of birth.[29][30] Of those with brain tumors, almost 30% have epilepsy, making them the cause of about 4% of cases.[50] The risk is greatest for tumors in the temporal lobe and those that grow slowly.[50] Other mass lesions such as cerebral cavernous malformations and arteriovenous malformations have risks as high as 40–60%.[50] Of those who have had a stroke, 2–4% develop epilepsy.[50] In the United Kingdom strokes account for 15% of cases and it is believed to be the cause in 30% of the elderly.[25][50] Between 6 and 20% of epilepsy is believed to be due to head trauma.[50] Mild brain injury increases the risk about two-fold while severe brain injury increases the risk seven-fold.[50] In those who have experienced a high-powered gunshot wound to the head, the risk is about 50%.[50]
Some evidence links epilepsy and celiac disease and non-celiac gluten sensitivity, while other evidence does not. There appears to be a specific syndrome which includes coeliac disease, epilepsy and calcifications in the brain.[51][52] A 2012 review estimates that between 1% and 6% of people with epilepsy have coeliac disease while 1% of the general population has the condition.[52]
The risk of epilepsy following meningitis is less than 10%; that disease more commonly causes seizures during the infection itself.[50] In herpes simplex encephalitis the risk of a seizure is around 50%[50] with a high risk of epilepsy following (up to 25%).[53][54] A form of an infection with the pork tapeworm (cysticercosis), in the brain, is known as neurocysticercosis, and is the cause of up to half of epilepsy cases in areas of the world where the parasite is common.[50] Epilepsy may also occur after other brain infections such as cerebral malaria, toxoplasmosis, and toxocariasis.[50] Chronic alcohol use increases the risk of epilepsy: those who drink six units of alcohol per day have a 2.5-fold increase in risk.[50] Other risks include Alzheimer's disease, multiple sclerosis, tuberous sclerosis, and autoimmune encephalitis.[50] Getting vaccinated does not increase the risk of epilepsy.[50] Malnutrition is a risk factor seen mostly in the developing world, although it is unclear however if it is a direct cause or an association.[19] People with cerebral palsy have an increased risk of epilepsy, with half of people with spastic quadriplegia and spastic hemiplegia having the disease.[55]
Mechanism
Normally brain electrical activity is non-synchronous, as neurons do not normally fire in sync with each other, but rather fire in order as signals travel throughout the brain.[3] Its activity is regulated by various factors both within the neuron and the cellular environment. Factors within the neuron include the type, number and distribution of ion channels, changes to receptors and changes of gene expression.[56] Factors around the neuron include ion concentrations, synaptic plasticity and regulation of transmitter breakdown by glial cells.[56][57] Chronic inflammation also appears to play a role.[58]
Epilepsy
The exact mechanism of epilepsy is unknown,[59] but a little is known about its cellular and network mechanisms. However, it is unknown under which circumstances the brain shifts into the activity of a seizure with its excessive synchronization.[60][61]
In epilepsy, the resistance of excitatory neurons to fire during this period is decreased.[3] This may occur due to changes in ion channels or inhibitory neurons not functioning properly.[3] This then results in a specific area from which seizures may develop, known as a "seizure focus".[3] Another mechanism of epilepsy may be the up-regulation of excitatory circuits or down-regulation of inhibitory circuits following an injury to the brain.[3][4] These secondary epilepsies occur through processes known as epileptogenesis.[3][4] Failure of the blood–brain barrier may also be a causal mechanism as it would allow substances in the blood to enter the brain.[62]
Seizures
There is evidence that epileptic seizures are usually not a random event. Seizures are often brought on by factors such as stress, alcohol abuse, flickering light, or a lack of sleep, among others. The term seizure threshold is used to indicate the amount of stimulus necessary to bring about a seizure. Seizure threshold is lowered in epilepsy.[60]
In epileptic seizures a group of neurons begin firing in an abnormal, excessive,[25] and synchronized manner.[3] This results in a wave of depolarization known as a paroxysmal depolarizing shift.[63] Normally, after an excitatory neuron fires it becomes more resistant to firing for a period of time.[3] This is due in part to the effect of inhibitory neurons, electrical changes within the excitatory neuron, and the negative effects of adenosine.[3]
Focal seizures begin in one hemisphere of the brain while generalized seizures begin in both hemispheres.[29] Some types of seizures may change brain structure, while others appear to have little effect.[64] Gliosis, neuronal loss, and atrophy of specific areas of the brain are linked to epilepsy but it is unclear if epilepsy causes these changes or if these changes result in epilepsy.[64]
Diagnosis

The diagnosis of epilepsy is typically made based on observation of the seizure onset and the underlying cause.[25] An electroencephalogram (EEG) to look for abnormal patterns of brain waves and neuroimaging (CT scan or MRI) to look at the structure of the brain are also usually part of the workup.[25] While figuring out a specific epileptic syndrome is often attempted, it is not always possible.[25] Video and EEG monitoring may be useful in difficult cases.[65]
Definition
Epilepsy is a disorder of the brain defined by any of the following conditions:[66]
- At least two unprovoked (or reflex) seizures occurring more than 24 hours apart
- One unprovoked (or reflex) seizure and a probability of further seizures similar to the general recurrence risk (at least 60%) after two unprovoked seizures, occurring over the next 10 years
- Diagnosis of an epilepsy syndrome
Furthermore, epilepsy is considered to be resolved for individuals who had an age-dependent epilepsy syndrome but are now past that age or those who have remained seizure-free for the last 10 years, with no seizure medicines for the last 5 years.[66]
This 2014 definition of the International League Against Epilepsy[66] is a clarification of the ILAE 2005 conceptual definition, according to which epilepsy is "a disorder of the brain characterized by an enduring predisposition to generate epileptic seizures and by the neurobiologic, cognitive, psychological, and social consequences of this condition. The definition of epilepsy requires the occurrence of at least one epileptic seizure."[12][67]
It is, therefore, possible to outgrow epilepsy or to undergo treatment that causes epilepsy to be resolved, but with no guarantee that it will not return. In the definition, epilepsy is now called a disease, rather than a disorder. This was a decision of the executive committee of the ILAE, taken because the word "disorder," while perhaps having less stigma than does "disease," also does not express the degree of seriousness that epilepsy deserves.[66]
The definition is practical in nature and is designed for clinical use. In particular, it aims to clarify when an "enduring predisposition" according to the 2005 conceptual definition is present. Researchers, statistically-minded epidemiologists, and other specialized groups may choose to use the older definition or a definition of their own devising. The ILAE considers doing so is perfectly allowable, so long as it is clear what definition is being used.[66]
Classification
In contrast to the classification of seizures which focuses on what happens during a seizure, the classification of epilepsies focuses on the underlying causes. When a person is admitted to hospital after an epileptic seizure the diagnostic workup results preferably in the seizure itself being classified (e.g. tonic-clonic) and in the underlying disease being identified (e.g. hippocampal sclerosis).[65] The name of the diagnosis finally made depends on the available diagnostic results and the applied definitions and classifications (of seizures and epilepsies) and its respective terminology.
The International League Against Epilepsy (ILAE) provided a classification of the epilepsies and epileptic syndromes in 1989 as follows:[68]
- Localization-related epilepsies and syndromes
- Unknown cause (e.g. benign childhood epilepsy with centrotemporal spikes)
- Symptomatic/cryptogenic (e.g. temporal lobe epilepsy)
- Generalized
- Unknown cause (e.g. childhood absence epilepsy)
- Cryptogenic or symptomatic (e.g. Lennox-Gastaut syndrome)
- Symptomatic (e.g. early infantile epileptic encephalopathy with burst suppression)
- Epilepsies and syndromes undetermined whether focal or generalized
- With both generalized and focal seizures (e.g. epilepsy with continuous spike-waves during slow wave sleep)
- Special syndromes (with situation-related seizures)
- Localization-related epilepsies and syndromes
This classification was widely accepted but has also been criticized mainly because the underlying causes of epilepsy (which are a major determinant of clinical course and prognosis) were not covered in detail.[69] In 2010 the ILAE Commission for Classification of the Epilepsies addressed this issue and divided epilepsies into three categories (genetic, structural/metabolic, unknown cause)[70] that were refined in their 2011 recommendation into four categories and a number of subcategories reflecting recent technologic and scientific advances.[71]
- Unknown cause (mostly genetic or presumed genetic origin)
- Pure epilepsies due to single gene disorders
- Pure epilepsies with complex inheritance
- Symptomatic (associated with gross anatomic or pathologic abnormalities)
- Mostly genetic or developmental causation
- Childhood epilepsy syndromes
- Progressive myoclonic epilepsies
- Neurocutaneous syndromes
- Other neurologic single gene disorders
- Disorders of chromosome function
- Developmental anomalies of cerebral structure
- Mostly acquired causes
- Hippocampal sclerosis
- Perinatal and infantile causes
- Cerebral trauma, tumor or infection
- Cerebrovascular disorders
- Cerebral immunologic disorders
- Degenerative and other neurologic conditions
- Mostly genetic or developmental causation
- Provoked (a specific systemic or environmental factor is the predominant cause of the seizures)
- Provoking factors
- Reflex epilepsies
- Cryptogenic (presumed symptomatic nature in which the cause has not been identified)[71]
- Unknown cause (mostly genetic or presumed genetic origin)
Syndromes
Cases of epilepsy may be organized into epilepsy syndromes by the specific features that are present. These features include the age that seizure begin, the seizure types, EEG findings, among others. Identifying an epilepsy syndrome is useful as it helps determine the underlying causes as well as what anti-seizure medication should be tried.[29][72]
The ability to categorize a case of epilepsy into a specific syndrome occurs more often with children since the onset of seizures is commonly early.[48] Less serious examples are benign rolandic epilepsy (2.8 per 100,000), childhood absence epilepsy (0.8 per 100,000) and juvenile myoclonic epilepsy (0.7 per 100,000).[48] Severe syndromes with diffuse brain dysfunction caused, at least partly, by some aspect of epilepsy, are also referred to as epileptic encephalopathies. These are associated with frequent seizures that are resistant to treatment and severe cognitive dysfunction, for instance Lennox–Gastaut syndrome and West syndrome.[73] Genetics is believed to play an important role in epilepsies by a number of mechanisms. Simple and complex modes of inheritance have been identified for some of them. However, extensive screening have failed to identify many single gene variants of large effect.[74] More recent exome and genome sequencing studies have begun to reveal a number of de novo gene mutations that are responsible for some epileptic encephalopathies, including CHD2 and SYNGAP1[75][76][77] and DNM1, GABBR2, FASN and RYR3.[78]
Syndromes in which causes are not clearly identified are difficult to match with categories of the current classification of epilepsy. Categorization for these cases was made somewhat arbitrarily.[71] The idiopathic (unknown cause) category of the 2011 classification includes syndromes in which the general clinical features and/or age specificity strongly point to a presumed genetic cause.[71] Some childhood epilepsy syndromes are included in the unknown cause category in which the cause is presumed genetic, for instance benign rolandic epilepsy. Others are included in symptomatic despite a presumed genetic cause (in at least in some cases), for instance Lennox-Gastaut syndrome.[71] Clinical syndromes in which epilepsy is not the main feature (e.g. Angelman syndrome) were categorized symptomatic but it was argued to include these within the category idiopathic.[71] Classification of epilepsies and particularly of epilepsy syndromes will change with advances in research.
Tests
An electroencephalogram (EEG) can assist in showing brain activity suggestive of an increased risk of seizures. It is only recommended for those who are likely to have had an epileptic seizure on the basis of symptoms. In the diagnosis of epilepsy, electroencephalography may help distinguish the type of seizure or syndrome present. In children it is typically only needed after a second seizure. It cannot be used to rule out the diagnosis and may be falsely positive in those without the disease. In certain situations it may be useful to perform the EEG while the affected individual is sleeping or sleep deprived.[65]
Diagnostic imaging by CT scan and MRI is recommended after a first non-febrile seizure to detect structural problems in and around the brain.[65] MRI is generally a better imaging test except when bleeding is suspected, for which CT is more sensitive and more easily available.[20] If someone attends the emergency room with a seizure but returns to normal quickly, imaging tests may be done at a later point.[20] If a person has a previous diagnosis of epilepsy with previous imaging, repeating the imaging is usually not needed even if there are subsequent seizures.[65][79]
For adults, the testing of electrolyte, blood glucose and calcium levels is important to rule out problems with these as causes.[65] An electrocardiogram can rule out problems with the rhythm of the heart.[65] A lumbar puncture may be useful to diagnose a central nervous system infection but is not routinely needed.[20] In children additional tests may be required such as urine biochemistry and blood testing looking for metabolic disorders.[65][80]
A high blood prolactin level within the first 20 minutes following a seizure may be useful to help confirm an epileptic seizure as opposed to psychogenic non-epileptic seizure.[81][82] Serum prolactin level is less useful for detecting focal seizures.[83] If it is normal an epileptic seizure is still possible[82] and a serum prolactin does not separate epileptic seizures from syncope.[84] It is not recommended as a routine part of the diagnosis of epilepsy.[65]
Differential diagnosis
Diagnosis of epilepsy can be difficult. A number of other conditions may present very similar signs and symptoms to seizures, including syncope, hyperventilation, migraines, narcolepsy, panic attacks and psychogenic non-epileptic seizures (PNES).[85][86] In particular a syncope can be accompanied by a short episode of convulsions.[87] Nocturnal frontal lobe epilepsy, often misdiagnosed as nightmares, was considered to be a parasomnia but later identified to be an epilepsy syndrome.[88] Attacks of the movement disorder paroxysmal dyskinesia may be taken for epileptic seizures.[89] The cause of a drop attack can be, among many others, an atonic seizure.[86]
Children may have behaviors that are easily mistaken for epileptic seizures but are not. These include breath-holding spells, bed wetting, night terrors, tics and shudder attacks.[86] Gastroesophageal reflux may cause arching of the back and twisting of the head to the side in infants, which may be mistaken for tonic-clonic seizures.[86]
Misdiagnosis is frequent (occurring in about 5 to 30% of cases).[25] Different studies showed that in many cases seizure-like attacks in apparent treatment-resistant epilepsy have a cardiovascular cause.[87][90] Approximately 20% of the people seen at epilepsy clinics have PNES[20] and of those who have PNES about 10% also have epilepsy;[91] separating the two based on the seizure episode alone without further testing is often difficult.[91]
Prevention
While many cases are not preventable, efforts to reduce head injuries, provide good care around the time of birth, and reduce environmental parasites such as the pork tapeworm may be effective.[30] Efforts in one part of Central America to decrease rates of pork tapeworm resulted in a 50% decrease in new cases of epilepsy.[19]
Management

Epilepsy is usually treated with daily medication once a second seizure has occurred,[25][65] while medication may be started after the first seizure in those at high risk for subsequent seizures.[65] Supporting people's self management of their condition may be useful.[92] In drug-resistant cases different management options may be looked at including a special diet, the implantation of a neurostimulator, or neurosurgery.
First aid
Rolling a person with an active tonic-clonic seizure onto their side and into the recovery position helps prevent fluids from getting into the lungs.[93] Putting fingers, a bite block or tongue depressor in the mouth is not recommended as it might make the person vomit or result in the rescuer being bitten.[27][93] Efforts should be taken to prevent further self-injury.[27] Spinal precautions are generally not needed.[93]
If a seizure lasts longer than 5 minutes or if there are more than two seizures in an hour without a return to a normal level of consciousness between them, it is considered a medical emergency known as status epilepticus.[65][94] This may require medical help to keep the airway open and protected;[65] a nasopharyngeal airway may be useful for this.[93] At home the recommended initial medication for seizure of a long duration is midazolam placed in the mouth.[95] Diazepam may also be used rectally.[95] In hospital, intravenous lorazepam is preferred.[65] If two doses of benzodiazepines are not effective, other medications such as phenytoin are recommended.[65] Convulsive status epilepticus that does not respond to initial treatment typically requires admission to the intensive care unit and treatment with stronger agents such as thiopentone or propofol.[65]
Medications

The mainstay treatment of epilepsy is anticonvulsant medications, possibly for the person's entire life.[25] The choice of anticonvulsant is based on seizure type, epilepsy syndrome, other medications used, other health problems, and the person's age and lifestyle.[95] A single medication is recommended initially;[96] if this is not effective, switching to a single other medication is recommended.[65] Two medications at once is recommended only if a single medication does not work.[65] In about half, the first agent is effective; a second single agent helps in about 13% and a third or two agents at the same time may help an additional 4%.[97] About 30% of people continue to have seizures despite anticonvulsant treatment.[8]
There are a number of medications available including phenytoin, carbamazepine and valproate. Evidence suggests that phenytoin, carbamazepine, and valproate may be equally effective in both focal and generalized seizures.[98][99] Controlled release carbamazepine appears to work as well as immediate release carbamazepine, and may have fewer side effects.[100] In the United Kingdom, carbamazepine or lamotrigine are recommended as first-line treatment for focal seizures, with levetiracetam and valproate as second-line due to issues of cost and side effects.[65] Valproate is recommended first-line for generalized seizures with lamotrigine being second-line.[65] In those with absence seizures, ethosuximide or valproate are recommended; valproate is particularly effective in myoclonic seizures and tonic or atonic seizures.[65] If seizures are well-controlled on a particular treatment, it is not usually necessary to routinely check the medication levels in the blood.[65]
The least expensive anticonvulsant is phenobarbital at around US$5 a year.[19] The World Health Organization gives it a first-line recommendation in the developing world and it is commonly used there.[101][102] Access however may be difficult as some countries label it as a controlled drug.[19]
Adverse effects from medications are reported in 10 to 90% of people, depending on how and from whom the data is collected.[103] Most adverse effects are dose-related and mild.[103] Some examples include mood changes, sleepiness, or an unsteadiness in gait.[103] Certain medications have side effects that are not related to dose such as rashes, liver toxicity, or suppression of the bone marrow.[103] Up to a quarter of people stop treatment due to adverse effects.[103] Some medications are associated with birth defects when used in pregnancy.[65] Many of the common used medications, such as valproate, phenytoin, carbamazepine, phenobarbitol, and gabapentin have been reported to cause increased risk of birth defects,[104] especially when used during the first trimester.[105] Despite this, treatment is often continued once effective, because the risk of untreated epilepsy is believed to be greater than the risk of the medications.[105] Among the antiepileptic medications, levetiracetam and lamotrigine seem to carry the lowest risk of causing birth defects.[104]
Slowly stopping medications may be reasonable in some people who do not have a seizure for two to four years; however, around a third of people have a recurrence, most often during the first six months.[65][106] Stopping is possible in about 70% of children and 60% of adults.[30] Measuring medication levels is not generally needed in those whose seizures are well controlled.[79]
Surgery
Epilepsy surgery may be an option for people with focal seizures that remain a problem despite other treatments.[107][108] These other treatments include at least a trial of two or three medications.[109] The goal of surgery is total control of seizures[110] and this may be achieved in 60–70% of cases.[109] Common procedures include cutting out the hippocampus via an anterior temporal lobe resection, removal of tumors, and removing parts of the neocortex.[109] Some procedures such as a corpus callosotomy are attempted in an effort to decrease the number of seizures rather than cure the condition.[109] Following surgery, medications may be slowly withdrawn in many cases.[109][107]
Neurostimulation may be another option in those who are not candidates for surgery.[65] Three types have been used in those who do not respond to medications: vagus nerve stimulation, anterior thalamic stimulation, and closed-loop responsive stimulation.[6][111][112]
Diet
There is promising evidence that a ketogenic diet (high-fat, low-carbohydrate, adequate-protein) decreases the number of seizures and eliminate seizures in some; however, further research is necessary.[7] It is a reasonable option in those who have epilepsy that is not improved with medications and for whom surgery is not an option.[7] About 10% stay on the diet for a few years due to issues of effectiveness and tolerability.[7] Side effects include stomach and intestinal problems in 30%, and there are long-term concerns about heart disease.[7] Less radical diets are easier to tolerate and may be effective.[7] It is unclear why this diet works.[113] In people with coeliac disease or non-celiac gluten sensitivity and occipital calcifications, a gluten-free diet may decrease the frequency of seizures.[52]
Other
Avoidance therapy consists of minimizing or eliminating triggers. For example, those who are sensitive to light may have success with using a small television, avoiding video games, or wearing dark glasses.[114] Operant-based biofeedback based on the EEG waves has some support in those who do not respond to medications.[115] Psychological methods should not, however, be used to replace medications.[65]
Exercise has been proposed as possibly useful for preventing seizures,[116] with some data to support this claim.[117] Some dogs, commonly referred to as seizure dogs, may help during or after a seizure.[118][119] It is not clear if dogs have the ability to predict seizures before they occur.[120]
There is moderate-quality evidence supporting the use of psychological interventions along with other treatments in epilepsy.[121] This can improve quality of life, enhance emotional wellbeing, and reduce fatigue in adults and adolescents.[121] Psychological interventions may also improve seizure control for some individuals by promoting self-management and adherence.[121]
As an add-on therapy in those who are not well controlled with other medications, cannabidiol appears to be useful in some children.[122] In 2018 the FDA approved this product for Lennox–Gastaut syndrome and Dravet syndrome.[123]
Alternative medicine
Alternative medicine, including acupuncture,[124] routine vitamins,[125] and yoga,[126] have no reliable evidence to support their use in epilepsy. Melatonin, as of 2016, is insufficiently supported by evidence.[127] The trials were of poor methodological quality and it was not possible to draw any definitive conclusions.[127]
Prognosis
Epilepsy cannot usually be cured, but medication can control seizures effectively in about 70% of cases.[8] Of those with generalized seizures, more than 80% can be well controlled with medications while this is true in only 50% of people with focal seizures.[6] One predictor of long-term outcome is the number of seizures that occur in the first six months.[25] Other factors increasing the risk of a poor outcome include little response to the initial treatment, generalized seizures, a family history of epilepsy, psychiatric problems, and waves on the EEG representing generalized epileptiform activity.[128] In the developing world, 75% of people are either untreated or not appropriately treated.[30] In Africa, 90% do not get treatment.[30] This is partly related to appropriate medications not being available or being too expensive.[30]
Mortality
People with epilepsy are at an increased risk of death.[129] This increase is between 1.6 and 4.1 fold greater than that of the general population.[130] The greatest increase in mortality from epilepsy is among the elderly.[130] Those with epilepsy due to an unknown cause have little increased risk.[130]
Mortality is often related to: the underlying cause of the seizures, status epilepticus, suicide, trauma, and sudden unexpected death in epilepsy (SUDEP).[129] Death from status epilepticus is primarily due to an underlying problem rather than missing doses of medications.[129] The risk of suicide is between 2 and 6 times higher in those with epilepsy;[131][132] the cause of this is unclear.[131] SUDEP appears to be partly related to the frequency of generalized tonic-clonic seizures[133] and accounts for about 15% of epilepsy-related deaths;[128] it is unclear how to decrease its risk.[133]
In the United Kingdom, it is estimated that 40–60% of deaths are possibly preventable.[25] In the developing world, many deaths are due to untreated epilepsy leading to falls or status epilepticus.[19]
Epidemiology
Epilepsy is one of the most common serious neurological disorders[134] affecting about 50 million people as of 2022.[1] It affects 1% of the population by age 20 and 3% of the population by age 75.[17] It is more common in males than females with the overall difference being small.[19][48] Most of those with the disorder (80%) are in low income populations[135] or the developing world.[30]
The estimated prevalence of active epilepsy (as of 2012) is in the range 3–10 per 1,000, with active epilepsy defined as someone with epilepsy who has had a least one unprovoked seizure in the last five years.[48][136] Epilepsy begins each year in 40–70 per 100,000 in developed countries and 80–140 per 100,000 in developing countries.[30] Poverty is a risk and includes both being from a poor country and being poor relative to others within one's country.[19] In the developed world epilepsy most commonly starts either in the young or in the old.[19] In the developing world its onset is more common in older children and young adults due to the higher rates of trauma and infectious diseases.[19] In developed countries the number of cases a year has decreased in children and increased among the elderly between the 1970s and 2003.[136] This has been attributed partly to better survival following strokes in the elderly.[48]
History
The oldest medical records show that epilepsy has been affecting people at least since the beginning of recorded history.[137] Throughout ancient history, the disease was thought to be a spiritual condition.[137] The world's oldest description of an epileptic seizure comes from a text in Akkadian (a language used in ancient Mesopotamia) and was written around 2000 BC.[23] The person described in the text was diagnosed as being under the influence of a moon god, and underwent an exorcism.[23] Epileptic seizures are listed in the Code of Hammurabi (c. 1790 BC) as reason for which a purchased slave may be returned for a refund,[23] and the Edwin Smith Papyrus (c. 1700 BC) describes cases of individuals with epileptic convulsions.[23]
The oldest known detailed record of the disease itself is in the Sakikku, a Babylonian cuneiform medical text from 1067–1046 BC.[137] This text gives signs and symptoms, details treatment and likely outcomes,[23] and describes many features of the different seizure types.[137] As the Babylonians had no biomedical understanding of the nature of disease, they attributed the seizures to possession by evil spirits and called for treating the condition through spiritual means.[137] Around 900 BC, Punarvasu Atreya described epilepsy as loss of consciousness;[138] this definition was carried forward into the Ayurvedic text of Charaka Samhita (about 400 BC).[139]
The ancient Greeks had contradictory views of the disease. They thought of epilepsy as a form of spiritual possession, but also associated the condition with genius and the divine. One of the names they gave to it was the sacred disease (ἠ ἱερὰ νόσος).[23][140] Epilepsy appears within Greek mythology: it is associated with the Moon goddesses Selene and Artemis, who afflicted those who upset them. The Greeks thought that important figures such as Julius Caesar and Hercules had the disease.[23] The notable exception to this divine and spiritual view was that of the school of Hippocrates. In the fifth century BC, Hippocrates rejected the idea that the disease was caused by spirits. In his landmark work On the Sacred Disease, he proposed that epilepsy was not divine in origin and instead was a medically treatable problem originating in the brain.[23][137] He accused those of attributing a sacred cause to the disease of spreading ignorance through a belief in superstitious magic.[23] Hippocrates proposed that heredity was important as a cause, described worse outcomes if the disease presents at an early age, and made note of the physical characteristics as well as the social shame associated with it.[23] Instead of referring to it as the sacred disease, he used the term great disease, giving rise to the modern term grand mal, used for tonic–clonic seizures.[23] Despite his work detailing the physical origins of the disease, his view was not accepted at the time.[137] Evil spirits continued to be blamed until at least the 17th century.[137]
In Ancient Rome people did not eat or drink with the same pottery as that used by someone who was affected.[141] People of the time would spit on their chest believing that this would keep the problem from affecting them.[141] According to Apuleius and other ancient physicians, in order to detect epilepsy, it was common to light a piece of gagates, whose smoke would trigger the seizure.[142] Occasionally a spinning potter's wheel was used, perhaps a reference to photosensitive epilepsy.[143]
In most cultures, persons with epilepsy have been stigmatized, shunned, or even imprisoned. As late as in the second half of the 20th century, in Tanzania and other parts of Africa epilepsy was associated with possession by evil spirits, witchcraft, or poisoning and was believed by many to be contagious.[144] In the Salpêtrière, the birthplace of modern neurology, Jean-Martin Charcot found people with epilepsy side by side with the mentally ill, those with chronic syphilis, and the criminally insane. In ancient Rome, epilepsy was known as the morbus comitialis ('disease of the assembly hall') and was seen as a curse from the gods. In northern Italy, epilepsy was once traditionally known as Saint Valentine's malady.[145]
In the mid-1800s, the first effective anti-seizure medication, bromide, was introduced.[103] The first modern treatment, phenobarbital, was developed in 1912, with phenytoin coming into use in 1938.[146]
Society and culture
Stigma
Stigma is commonly experienced, around the world, by those with epilepsy.[147] It can affect people economically, socially and culturally.[147] In India and China, epilepsy may be used as justification to deny marriage.[30] People in some areas still believe those with epilepsy to be cursed.[19] In parts of Africa, such as Tanzania and Uganda, epilepsy is incorrectly claimed to be associated with possession by evil spirits, witchcraft, or poisoning and is believed by many to be contagious.[144][19] Before 1971 in the United Kingdom, epilepsy was considered grounds for the annulment of marriage.[30] The stigma may result in some people with epilepsy denying that they have ever had seizures.[48]
Economics
Seizures result in direct economic costs of about one billion dollars in the United States.[20] Epilepsy resulted in economic costs in Europe of around 15.5 billion Euros in 2004.[25] In India epilepsy is estimated to result in costs of US$1.7 billion or 0.5% of the GDP.[30] It is the cause of about 1% of emergency department visits (2% for emergency departments for children) in the United States.[148]
Vehicles
Those with epilepsy are at about twice the risk of being involved in a motor vehicular collision and thus in many areas of the world are not allowed to drive or only able to drive if certain conditions are met.[22] In some places physicians are required by law to report if a person has had a seizure to the licensing body while in others the requirement is only that they encourage the person in question to report it themselves.[22] Countries that require physician reporting include Sweden, Austria, Denmark and Spain.[22] Countries that require the individual to report include the UK and New Zealand and the physician may report if they believe the individual has not already.[22] In Canada, the United States and Australia the requirements around reporting vary by province or state.[22] If seizures are well controlled most feel allowing driving is reasonable.[149] The amount of time a person must be free from seizures before they can drive varies by country.[149] Many countries require one to three years without seizures.[149] In the United States the time needed without a seizure is determined by each state and is between three months and one year.[149]
Those with epilepsy or seizures are typically denied a pilot license.[150] In Canada if an individual has had no more than one seizure, they may be considered after five years for a limited license if all other testing is normal.[151] Those with febrile seizures and drug related seizures may also be considered.[151] In the United States, the Federal Aviation Administration does not allow those with epilepsy to get a commercial pilot license.[152] Rarely, exceptions can be made for persons who have had an isolated seizure or febrile seizures and have remained free of seizures into adulthood without medication.[153] In the United Kingdom, a full national private pilot license requires the same standards as a professional driver's license.[154] This requires a period of ten years without seizures while off medications.[155] Those who do not meet this requirement may acquire a restricted license if free from seizures for five years.[154]
Support organizations
There are organizations that provide support for people and families affected by epilepsy. The Out of the Shadows campaign, a joint effort by the World Health Organization, the International League Against Epilepsy and the International Bureau for Epilepsy, provides help internationally.[30] In the United States, the Epilepsy Foundation is a national organization that works to increase the acceptance of those with the disorder, their ability to function in society and to promote research for a cure.[156] The Epilepsy Foundation, some hospitals, and some individuals also run support groups in the United States.[157]
International Epilepsy Day (World Epilepsy Day) began in 2015 and occurs on the second Monday in February.[158][159]
Research
Seizure prediction and modeling
Seizure prediction refers to attempts to forecast epileptic seizures based on the EEG before they occur.[160] As of 2011, no effective mechanism to predict seizures has been developed.[160] Kindling, where repeated exposures to events that could cause seizures eventually causes seizures more easily, has been used to create animal models of epilepsy.[161]
Potential future therapies
Gene therapy is being studied in some types of epilepsy.[162] Medications that alter immune function, such as intravenous immunoglobulins, are poorly supported by evidence.[163] Noninvasive stereotactic radiosurgery is, as of 2012, being compared to standard surgery for certain types of epilepsy.[164]
Other animals
Epilepsy occurs in a number of other animals including dogs and cats and is the most common brain disorder in dogs.[165] It is typically treated with anticonvulsants such as phenobarbital or bromide in dogs and phenobarbital in cats.[165] Imepitoin is also used in dogs.[166] While generalized seizures in horses are fairly easy to diagnose, it may be more difficult in non-generalized seizures and EEGs may be useful.[167]
References
- 1 2 3 4 5 6 "Epilepsy". www.who.int. World Health Organization. Archived from the original on 3 June 2022. Retrieved 3 June 2022.
- 1 2 3 4 5 6 7 8 9 "Epilepsy Fact sheet". WHO. February 2016. Archived from the original on 11 March 2016. Retrieved 4 March 2016.
- 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 Hammer, Gary D.; McPhee, Stephen J., eds. (2010). "7". Pathophysiology of disease : an introduction to clinical medicine (6th ed.). New York: McGraw-Hill Medical. ISBN 978-0-07-162167-0.
- 1 2 3 4 Goldberg EM, Coulter DA (May 2013). "Mechanisms of epileptogenesis: a convergence on neural circuit dysfunction". Nature Reviews. Neuroscience. 14 (5): 337–49. doi:10.1038/nrn3482. PMC 3982383. PMID 23595016.
- 1 2 3 4 5 6 Longo, Dan L (2012). "369 Seizures and Epilepsy". Harrison's principles of internal medicine (18th ed.). McGraw-Hill. p. 3258. ISBN 978-0-07-174887-2.
- 1 2 3 4 Bergey GK (June 2013). "Neurostimulation in the treatment of epilepsy". Experimental Neurology. 244: 87–95. doi:10.1016/j.expneurol.2013.04.004. PMID 23583414.
- 1 2 3 4 5 6 7 Martin-McGill, Kirsty J.; Jackson, Cerian F.; Bresnahan, Rebecca; Levy, Robert G.; Cooper, Paul N. (7 November 2018). "Ketogenic diets for drug-resistant epilepsy". The Cochrane Database of Systematic Reviews. 11: CD001903. doi:10.1002/14651858.CD001903.pub4. ISSN 1469-493X. PMC 6517043. PMID 30403286.
- 1 2 3 4 Eadie MJ (December 2012). "Shortcomings in the current treatment of epilepsy". Expert Review of Neurotherapeutics. 12 (12): 1419–27. doi:10.1586/ern.12.129. PMID 23237349.
- 1 2 Wang, Haidong; Naghavi, Mohsen; Allen, Christine; Barber, Ryan M.; Bhutta, Zulfiqar A.; Carter, Austin; Casey, Daniel C.; Charlson, Fiona J.; Chen, Alan Zian; Coates, Matthew M.; Coggeshall, Megan; Dandona, Lalit; Dicker, Daniel J.; Erskine, Holly E.; Ferrari, Alize J.; Fitzmaurice, Christina; Foreman, Kyle; Forouzanfar, Mohammad H.; Fraser, Maya S.; Fullman, Nancy; Gething, Peter W.; Goldberg, Ellen M.; Graetz, Nicholas; Haagsma, Juanita A.; Hay, Simon I.; Huynh, Chantal; Johnson, Catherine O.; Kassebaum, Nicholas J.; Kinfu, Yohannes; Kulikoff, Xie Rachel (October 2016). "Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980-2015: a systematic analysis for the Global Burden of Disease Study 2015". Lancet. 388 (10053): 1459–1544. doi:10.1016/s0140-6736(16)31012-1. PMC 5388903. PMID 27733281.
{{cite journal}}: Unknown parameter|displayauthors=ignored (help) - ↑ Wiebe, Samuel (2020). "375. The epilepsies". In Goldman, Lee; Schafer, Andrew I. (eds.). Goldman-Cecil Medicine. Vol. 2 (26th ed.). Philadelphia: Elsevier. pp. 2358–2370. ISBN 978-0-323-53266-2. Archived from the original on 11 June 2022. Retrieved 3 June 2022.
- ↑ Chang BS, Lowenstein DH (September 2003). "Epilepsy". The New England Journal of Medicine. 349 (13): 1257–66. doi:10.1056/NEJMra022308. PMID 14507951.
- 1 2 3 Fisher R, van Emde Boas W, Blume W, Elger C, Genton P, Lee P, Engel J (2005). "Epileptic seizures and epilepsy: definitions proposed by the International League Against Epilepsy (ILAE) and the International Bureau for Epilepsy (IBE)". Epilepsia. 46 (4): 470–2. doi:10.1111/j.0013-9580.2005.66104.x. PMID 15816939.
- 1 2 3 4 5 6 7 Pandolfo, M. (Nov 2011). "Genetics of epilepsy". Seminars in Neurology. 31 (5): 506–18. doi:10.1055/s-0031-1299789. PMID 22266888.
- ↑ Fiest, KM; Sauro, KM; Wiebe, S; Patten, SB; Kwon, CS; Dykeman, J; Pringsheim, T; Lorenzetti, DL; Jetté, N (17 January 2017). "Prevalence and incidence of epilepsy: A systematic review and meta-analysis of international studies". Neurology. 88 (3): 296–303. doi:10.1212/WNL.0000000000003509. PMID 27986877.
- ↑ GBD 2013 Mortality Causes of Death Collaborators (January 2015). "Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990-2013: a systematic analysis for the Global Burden of Disease Study 2013". Lancet. 385 (9963): 117–71. doi:10.1016/S0140-6736(14)61682-2. PMC 4340604. PMID 25530442. Archived from the original on 10 March 2021. Retrieved 15 July 2020.
- ↑ Brodie MJ, Elder AT, Kwan P (November 2009). "Epilepsy in later life". The Lancet. Neurology. 8 (11): 1019–30. doi:10.1016/S1474-4422(09)70240-6. PMID 19800848.
- 1 2 Holmes, Thomas R.; Browne, Gregory L. (2008). Handbook of epilepsy (4th ed.). Philadelphia: Lippincott Williams & Wilkins. p. 7. ISBN 978-0-7817-7397-3. Archived from the original on 31 March 2021. Retrieved 15 July 2020.
- ↑ Wyllie's treatment of epilepsy : principles and practice (5th ed.). Philadelphia: Wolters Kluwer/Lippincott Williams & Wilkins. 2010. ISBN 978-1-58255-937-7. Archived from the original on 24 June 2016.
- 1 2 3 4 5 6 7 8 9 10 11 12 Newton CR, Garcia HH (September 2012). "Epilepsy in poor regions of the world". Lancet. 380 (9848): 1193–201. doi:10.1016/S0140-6736(12)61381-6. PMID 23021288.
- 1 2 3 4 5 6 Wilden JA, Cohen-Gadol AA (August 2012). "Evaluation of first nonfebrile seizures". American Family Physician. 86 (4): 334–40. PMID 22963022.
- ↑ Berg AT (2008). "Risk of recurrence after a first unprovoked seizure". Epilepsia. 49 Suppl 1: 13–8. doi:10.1111/j.1528-1167.2008.01444.x. PMID 18184149.
- 1 2 3 4 5 6 L Devlin A, Odell M, L Charlton J, Koppel S (December 2012). "Epilepsy and driving: current status of research". Epilepsy Research. 102 (3): 135–52. doi:10.1016/j.eplepsyres.2012.08.003. PMID 22981339.
- 1 2 3 4 5 6 7 8 9 10 11 12 Magiorkinis E, Sidiropoulou K, Diamantis A (January 2010). "Hallmarks in the history of epilepsy: epilepsy in antiquity". Epilepsy & Behavior. 17 (1): 103–8. doi:10.1016/j.yebeh.2009.10.023. PMID 19963440.
- 1 2 Duncan JS, Sander JW, Sisodiya SM, Walker MC (April 2006). "Adult epilepsy" (PDF). Lancet. 367 (9516): 1087–1100. doi:10.1016/S0140-6736(06)68477-8. PMID 16581409. Archived from the original (PDF) on 24 March 2013. Retrieved 10 January 2012.
- 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 National Clinical Guideline Centre (January 2012). The Epilepsies: The diagnosis and management of the epilepsies in adults and children in primary and secondary care (PDF). National Institute for Health and Clinical Excellence. pp. 21–28. Archived (PDF) from the original on 16 December 2013.
- ↑ Hughes, JR (August 2009). "Absence seizures: a review of recent reports with new concepts". Epilepsy & Behavior. 15 (4): 404–12. doi:10.1016/j.yebeh.2009.06.007. PMID 19632158.
- 1 2 3 4 Shearer, Peter. "Seizures and Status Epilepticus: Diagnosis and Management in the Emergency Department". Emergency Medicine Practice. Archived from the original on 30 December 2010.
- 1 2 3 4 Bradley, Walter G. (2012). "67". Bradley's neurology in clinical practice (6th ed.). Philadelphia, PA: Elsevier/Saunders. ISBN 978-1-4377-0434-1.
- 1 2 3 4 5 National Clinical Guideline Centre (January 2012). The Epilepsies: The diagnosis and management of the epilepsies in adults and children in primary and secondary care (PDF). National Institute for Health and Clinical Excellence. pp. 119–129. Archived (PDF) from the original on 16 December 2013.
- 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 "Epilepsy". Fact Sheets. World Health Organization. October 2012. Archived from the original on 11 March 2016. Retrieved 24 January 2013.
- 1 2 3 Engel, Jerome (2008). Epilepsy : a comprehensive textbook (2nd ed.). Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins. p. 2797. ISBN 978-0-7817-5777-5. Archived from the original on 20 May 2016.
- 1 2 Simon, David A.; Greenberg, Michael J.; Aminoff, Roger P. (2012). "12". Clinical neurology (8th ed.). New York: McGraw-Hill Medical. ISBN 978-0-07-175905-2.
- 1 2 Steven C. Schachter, ed. (2008). Behavioral aspects of epilepsy : principles and practice ([Online-Ausg.]. ed.). New York: Demos. p. 125. ISBN 978-1-933864-04-4. Archived from the original on 1 August 2020. Retrieved 15 July 2020.
- ↑ Xue LY, Ritaccio AL (March 2006). "Reflex seizures and reflex epilepsy". American Journal of Electroneurodiagnostic Technology. 46 (1): 39–48. doi:10.1080/1086508X.2006.11079556. PMID 16605171.
- ↑ Malow BA (November 2005). "Sleep and epilepsy". Neurologic Clinics. 23 (4): 1127–47. doi:10.1016/j.ncl.2005.07.002. PMID 16243619.
- ↑ Tinuper P, Provini F, Bisulli F, Vignatelli L, Plazzi G, Vetrugno R, Montagna P, Lugaresi E (August 2007). "Movement disorders in sleep: guidelines for differentiating epileptic from non-epileptic motor phenomena arising from sleep". Sleep Medicine Reviews. 11 (4): 255–67. doi:10.1016/j.smrv.2007.01.001. PMID 17379548.
- ↑ Holmes, Thomas R. (2008). Handbook of epilepsy (4th ed.). Philadelphia: Lippincott Williams & Wilkins. p. 34. ISBN 978-0-7817-7397-3. Archived from the original on 1 August 2020. Retrieved 15 July 2020.
- 1 2 3 Panayiotopoulos CP (2010). A clinical guide to epileptic syndromes and their treatment based on the ILAE classifications and practice parameter guidelines (Rev. 2nd ed.). London: Springer. p. 445. ISBN 978-1-84628-644-5. Archived from the original on 1 August 2020. Retrieved 15 July 2020.
- ↑ Wheless JW, ed. (2009). Advanced therapy in epilepsy. Shelton, Conn.: People's Medical Pub. House. p. 443. ISBN 978-1-60795-004-2. Archived from the original on 1 August 2020. Retrieved 15 July 2020.
- ↑ Larner, Andrew J. (2010). A dictionary of neurological signs (3rd ed.). New York: Springer. p. 348. ISBN 978-1-4419-7095-4. Archived from the original on 1 August 2020. Retrieved 15 July 2020.
- ↑ Kaplan PW (November 2011). "Obsessive-compulsive disorder in chronic epilepsy". Epilepsy & Behavior. 22 (3): 428–32. doi:10.1016/j.yebeh.2011.07.029. PMID 21889913. Archived from the original on 14 December 2019. Retrieved 15 July 2020.
- ↑ Stefan, Hermann (2012). Epilepsy Part I: Basic Principles and Diagnosis E-Book: Handbook of Clinical Neurology (Volume 107 of Handbook of Clinical Neurology ed.). Newnes. p. 471. ISBN 978-0-444-53505-4. Archived from the original on 1 August 2020. Retrieved 15 July 2020.
- ↑ Plioplys S, Dunn DW, Caplan R (November 2007). "10-year research update review: psychiatric problems in children with epilepsy". Journal of the American Academy of Child and Adolescent Psychiatry. 46 (11): 1389–402. doi:10.1097/chi.0b013e31815597fc. PMID 18049289.
- ↑ Reilly CJ (May–June 2011). "Attention deficit hyperactivity disorder (ADHD) in childhood epilepsy". Research in Developmental Disabilities. 32 (3): 883–93. doi:10.1016/j.ridd.2011.01.019. PMID 21310586.
- ↑ Levisohn PM (2007). "The autism-epilepsy connection". Epilepsia. 48 Suppl 9 (Suppl 9): 33–5. doi:10.1111/j.1528-1167.2007.01399.x. PMID 18047599.
- 1 2 3 Berkovic SF, Mulley JC, Scheffer IE, Petrou S (2006). "Human epilepsies: interaction of genetic and acquired factors". Trends in Neurosciences. 29 (7): 391–7. doi:10.1016/j.tins.2006.05.009. PMID 16769131.
- ↑ Thurman DJ, Beghi E, Begley CE, Berg AT, Buchhalter JR, Ding D, Hesdorffer DC, Hauser WA, Kazis L, Kobau R, Kroner B, Labiner D, Liow K, Logroscino G, Medina MT, Newton CR, Parko K, Paschal A, Preux PM, Sander JW, Selassie A, Theodore W, Tomson T, Wiebe S, ILAE Commission on Epidemiology (September 2011). "Standards for epidemiologic studies and surveillance of epilepsy". Epilepsia. 52 Suppl 7: 2–26. doi:10.1111/j.1528-1167.2011.03121.x. PMID 21899536.
- 1 2 3 4 5 6 7 Neligan A, Hauser WA, Sander JW (2012). "The epidemiology of the epilepsies". Epilepsy. Handbook of Clinical Neurology. Vol. 107. pp. 113–33. doi:10.1016/B978-0-444-52898-8.00006-9. ISBN 978-0-444-52898-8. PMID 22938966.
- ↑ Dhavendra Kumar, ed. (2008). Genomics and clinical medicine. Oxford: Oxford University Press. p. 279. ISBN 978-0-19-972005-7. Archived from the original on 21 May 2016.
- 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 Bhalla D, Godet B, Druet-Cabanac M, Preux PM (June 2011). "Etiologies of epilepsy: a comprehensive review". Expert Review of Neurotherapeutics. 11 (6): 861–76. doi:10.1586/ern.11.51. PMID 21651333.
- ↑ Grossman G (April 2008). "Neurological complications of coeliac disease: what is the evidence?". Practical Neurology. 8 (2): 77–89. doi:10.1136/jnnp.2007.139717. PMID 18344378.
- 1 2 3 Jackson JR, Eaton WW, Cascella NG, Fasano A, Kelly DL (March 2012). "Neurologic and psychiatric manifestations of celiac disease and gluten sensitivity". The Psychiatric Quarterly. 83 (1): 91–102. doi:10.1007/s11126-011-9186-y. PMC 3641836. PMID 21877216.
- ↑ Shorvon, Simon D. (2011). The Causes of Epilepsy: Common and Uncommon Causes in Adults and Children. Cambridge University Press. p. 467. ISBN 978-1-139-49578-3. Archived from the original on 1 August 2020. Retrieved 15 July 2020.
- ↑ Sellner J, Trinka E (October 2012). "Seizures and epilepsy in herpes simplex virus encephalitis: current concepts and future directions of pathogenesis and management". Journal of Neurology. 259 (10): 2019–30. doi:10.1007/s00415-012-6494-6. PMID 22527234.
- ↑ Hadjipanayis A, Hadjichristodoulou C, Youroukos S (October 1997). "Epilepsy in patients with cerebral palsy". Developmental Medicine and Child Neurology. 39 (10): 659–63. doi:10.1111/j.1469-8749.1997.tb07359.x. PMID 9352726.
- 1 2 Bromfield EB (2006). An Introduction to Epilepsy. American Epilepsy Society. Archived from the original on 8 September 2017. Retrieved 15 July 2020.
- ↑ Blumenfeld H (2005). "Cellular and network mechanisms of spike-wave seizures". Epilepsia. 46 Suppl 9 (Suppl.9): 21–33. doi:10.1111/j.1528-1167.2005.00311.x. PMID 16302873.
- ↑ Rana A, Musto AE (May 2018). "The role of inflammation in the development of epilepsy". Journal of Neuroinflammation. 15 (1): 144. doi:10.1186/s12974-018-1192-7. PMC 5952578. PMID 29764485.
- ↑ Noebels, Jeffrey L.; Avoli, Massimo (2012-06-29). Jasper's Basic Mechanisms of the Epilepsies. Oxford University Press. pp. 466, 470. ISBN 9780199746545. Archived from the original on 1 August 2020. Retrieved 2014-10-16.
- 1 2 Le Van Quyen M, Navarro V, Martinerie J, Baulac M, Varela FJ (2003). "Toward a neurodynamical understanding of ictogenesis". Epilepsia. 44 Suppl 12 (Suppl.12): 30–43. doi:10.1111/j.0013-9580.2003.12007.x. PMID 14641559.
- ↑ Lopes da Silva F, Blanes W, Kalitzin SN, Parra J, Suffczynski P, Velis DN (2003). "Epilepsies as dynamical diseases of brain systems: basic models of the transition between normal and epileptic activity". Epilepsia. 44 Suppl 12 (Suppl.12): 72–83. doi:10.1111/j.0013-9580.2003.12005.x. PMID 14641563.
- ↑ Oby E, Janigro D (November 2006). "The blood-brain barrier and epilepsy". Epilepsia. 47 (11): 1761–74. doi:10.1111/j.1528-1167.2006.00817.x. PMID 17116015.
- ↑ Somjen, George G. (2004). Ions in the Brain Normal Function, Seizures, and Stroke. New York: Oxford University Press. p. 167. ISBN 978-0-19-803459-9. Archived from the original on 1 August 2020. Retrieved 15 July 2020.
- 1 2 Engel J, Pedley TA, eds. (2008). Epilepsy : a comprehensive textbook (2nd ed.). Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins. p. 483. ISBN 978-0-7817-5777-5. Archived from the original on 1 August 2020. Retrieved 15 July 2020.
- 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 National Clinical Guideline Centre (January 2012). The Epilepsies: The diagnosis and management of the epilepsies in adults and children in primary and secondary care (PDF). National Institute for Health and Clinical Excellence. pp. 57–83. Archived (PDF) from the original on 16 December 2013.
- 1 2 3 4 5 Fisher RS, Acevedo C, Arzimanoglou A, Bogacz A, Cross JH, Elger CE, Engel J, Forsgren L, French JA, Glynn M, Hesdorffer DC, Lee BI, Mathern GW, Moshé SL, Perucca E, Scheffer IE, Tomson T, Watanabe M, Wiebe S (April 2014). "ILAE official report: a practical clinical definition of epilepsy" (PDF). Epilepsia. 55 (4): 475–82. doi:10.1111/epi.12550. PMID 24730690. Archived from the original (PDF) on 9 June 2014.
- ↑ Panayiotopoulos, CP (December 2011). "The new ILAE report on terminology and concepts for organization of epileptic seizures: a clinician's critical view and contribution". Epilepsia. 52 (12): 2155–60. doi:10.1111/j.1528-1167.2011.03288.x. PMID 22004554.
- ↑ "Proposal for revised classification of epilepsies and epileptic syndromes. Commission on Classification and Terminology of the International League Against Epilepsy". Epilepsia. 30 (4): 389–99. 1989. doi:10.1111/j.1528-1157.1989.tb05316.x. PMID 2502382.
- ↑ Engel J (August 2006). "ILAE classification of epilepsy syndromes". Epilepsy Research. 70 Suppl 1 (Suppl 1): S5–10. doi:10.1016/j.eplepsyres.2005.11.014. PMID 16822650.
- ↑ Berg AT, Berkovic SF, Brodie MJ, Buchhalter J, Cross JH, van Emde Boas W, Engel J, French J, Glauser TA, Mathern GW, Moshé SL, Nordli D, Plouin P, Scheffer IE (April 2010). "Revised terminology and concepts for organization of seizures and epilepsies: report of the ILAE Commission on Classification and Terminology, 2005-2009". Epilepsia. 51 (4): 676–85. doi:10.1111/j.1528-1167.2010.02522.x. PMID 20196795.
- 1 2 3 4 5 6 Shorvon SD (June 2011). "The etiologic classification of epilepsy". Epilepsia. 52 (6): 1052–7. doi:10.1111/j.1528-1167.2011.03041.x. PMID 21449936.
- ↑ "Epilepsy syndromes". International league against epilepsy. Archived from the original on 6 October 2014. Retrieved 2014-10-06.
- ↑ Nordli DR (October 2012). "Epileptic encephalopathies in infants and children". Journal of Clinical Neurophysiology. 29 (5): 420–4. doi:10.1097/WNP.0b013e31826bd961. PMID 23027099.
- ↑ Heinzen EL, Depondt C, Cavalleri GL, Ruzzo EK, Walley NM, Need AC, et al. (August 2012). "Exome sequencing followed by large-scale genotyping fails to identify single rare variants of large effect in idiopathic generalized epilepsy". American Journal of Human Genetics. 91 (2): 293–302. doi:10.1016/j.ajhg.2012.06.016. PMC 3415540. PMID 22863189.
- ↑ Carvill GL, Heavin SB, Yendle SC, McMahon JM, O'Roak BJ, Cook J, et al. (July 2013). "Targeted resequencing in epileptic encephalopathies identifies de novo mutations in CHD2 and SYNGAP1". Nature Genetics. 45 (7): 825–30. doi:10.1038/ng.2646. PMC 3704157. PMID 23708187.
- ↑ Chénier S, Yoon G, Argiropoulos B, Lauzon J, Laframboise R, Ahn JW, et al. (2014). "CHD2 haploinsufficiency is associated with developmental delay, intellectual disability, epilepsy and neurobehavioural problems". Journal of Neurodevelopmental Disorders. 6 (1): 9. doi:10.1186/1866-1955-6-9. PMC 4022362. PMID 24834135.
- ↑ Suls A, Jaehn JA, Kecskés A, Weber Y, Weckhuysen S, Craiu DC, et al. (November 2013). "De novo loss-of-function mutations in CHD2 cause a fever-sensitive myoclonic epileptic encephalopathy sharing features with Dravet syndrome". American Journal of Human Genetics. 93 (5): 967–75. doi:10.1016/j.ajhg.2013.09.017. PMC 3824114. PMID 24207121.
- ↑ EuroEPINOMICS-RES Consortium (October 2014). "De novo mutations in synaptic transmission genes including DNM1 cause epileptic encephalopathies". American Journal of Human Genetics. 95 (4): 360–70. doi:10.1016/j.ajhg.2014.08.013. PMC 4185114. PMID 25262651.
- 1 2 "American Epilepsy Society Choosing Wisely". www.choosingwisely.org. Archived from the original on 31 August 2018. Retrieved 30 August 2018.
- ↑ Wallace, Sheila J.; Farrell, Kevin, eds. (2004). Epilepsy in children (2nd ed.). London: Arnold. p. 354. ISBN 978-0-340-80814-6. Archived from the original on 1 August 2020. Retrieved 15 July 2020.
- ↑ Luef, G (October 2010). "Hormonal alterations following seizures". Epilepsy & Behavior. 19 (2): 131–3. doi:10.1016/j.yebeh.2010.06.026. PMID 20696621.
- 1 2 Ahmad S, Beckett MW (2004). "Value of serum prolactin in the management of syncope". Emergency Medicine Journal. 21 (2): 3e–3. doi:10.1136/emj.2003.008870. PMC 1726305. PMID 14988379.
- ↑ Shukla G, Bhatia M, Vivekanandhan S, et al. (2004). "Serum prolactin levels for differentiation of nonepileptic versus true seizures: limited utility". Epilepsy & Behavior. 5 (4): 517–21. doi:10.1016/j.yebeh.2004.03.004. PMID 15256189.
- ↑ Chen DK, So YT, Fisher RS (2005). "Use of serum prolactin in diagnosing epileptic seizures: report of the Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology". Neurology. 65 (5): 668–75. doi:10.1212/01.wnl.0000178391.96957.d0. PMID 16157897.
- ↑ Brodtkorb E (2013). "Common imitators of epilepsy". Acta Neurologica Scandinavica. Supplementum. 127 (196): 5–10. doi:10.1111/ane.12043. PMID 23190285.
- 1 2 3 4 Marx, John A., ed. (2010). Rosen's emergency medicine : concepts and clinical practice (7th ed.). Philadelphia: Mosby/Elsevier. p. 2228. ISBN 978-0-323-05472-0. Archived from the original on 1 August 2020. Retrieved 15 July 2020.
- 1 2 Zaidi A, Clough P, Cooper P, Scheepers B, Fitzpatrick AP (July 2000). "Misdiagnosis of epilepsy: many seizure-like attacks have a cardiovascular cause". Journal of the American College of Cardiology. 36 (1): 181–4. doi:10.1016/S0735-1097(00)00700-2. PMID 10898432.
- ↑ Bisulli F, Vignatelli L, Provini F, Leta C, Lugaresi E, Tinuper P (December 2011). "Parasomnias and nocturnal frontal lobe epilepsy (NFLE): lights and shadows--controversial points in the differential diagnosis". Sleep Medicine. 12 Suppl 2 (Suppl2): S27–32. doi:10.1016/j.sleep.2011.10.008. PMID 22136895.
- ↑ Zhou JQ, Zhou LM, Fang ZY, Wang Q, Chen ZY, Yang LB, Chen SD, Cai XD (January 2011). "Analyzing clinical and electrophysiological characteristics of Paroxysmal Dyskinesia". Journal of Research in Medical Sciences. 16 (1): 110–4. PMC 3063430. PMID 21448393.
- ↑ Akhtar MJ (March 2002). "All seizures are not epilepsy: many have a cardiovascular cause". JPMA. The Journal of the Pakistan Medical Association. 52 (3): 116–20. PMID 12071066.
- 1 2 Jerome, Engel (2013). Seizures and epilepsy (2nd ed.). New York: Oxford University Press. p. 462. ISBN 9780195328547. Archived from the original on 1 August 2020. Retrieved 15 July 2020.
- ↑ Helmers SL, Kobau R, Sajatovic M, Jobst BC, Privitera M, Devinsky O, Labiner D, Escoffery C, Begley CE, Shegog R, Pandey D, Fraser RT, Johnson EK, Thompson NJ, Horvath KJ (March 2017). "Self-management in epilepsy: Why and how you should incorporate self-management in your practice". Epilepsy & Behavior. 68: 220–224. doi:10.1016/j.yebeh.2016.11.015. PMC 5381244. PMID 28202408.
- 1 2 3 4 Michael GE, O'Connor RE (February 2011). "The diagnosis and management of seizures and status epilepticus in the prehospital setting". Emergency Medicine Clinics of North America. 29 (1): 29–39. doi:10.1016/j.emc.2010.08.003. PMID 21109100.
- ↑ Wheless, James W.; Willmore, James; Brumback, Roger A. (2009). Advanced therapy in epilepsy. Shelton, Conn.: People's Medical Pub. House. p. 144. ISBN 9781607950042. Archived from the original on 1 August 2020. Retrieved 15 July 2020.
- 1 2 3 National Clinical Guideline Centre (January 2012). The Epilepsies: The diagnosis and management of the epilepsies in adults and children in primary and secondary care (PDF). National Institute for Health and Clinical Excellence. Archived (PDF) from the original on 16 December 2013.
- ↑ Wyllie, Elaine (2012). Wyllie's Treatment of Epilepsy: Principles and Practice. Lippincott Williams & Wilkins. p. 187. ISBN 978-1-4511-5348-4. Archived from the original on 1 August 2020. Retrieved 15 July 2020.
- ↑ Flanagan SR, Zaretsky H, Moroz A, eds. (2010). Medical aspects of disability; a handbook for the rehabilitation professional (4th ed.). New York: Springer. p. 182. ISBN 978-0-8261-2784-6. Archived from the original on 1 August 2020. Retrieved 15 July 2020.
- ↑ Nevitt, SJ; Marson, AG; Tudur Smith, C (18 July 2019). "Carbamazepine versus phenytoin monotherapy for epilepsy: an individual participant data review". The Cochrane Database of Systematic Reviews. 7: CD001911. doi:10.1002/14651858.CD001911.pub4. PMC 6637502. PMID 31318037.
- ↑ Nevitt, SJ; Marson, AG; Weston, J; Tudur Smith, C (9 August 2018). "Sodium valproate versus phenytoin monotherapy for epilepsy: an individual participant data review". The Cochrane Database of Systematic Reviews. 8: CD001769. doi:10.1002/14651858.CD001769.pub4. PMC 6513104. PMID 30091458.
- ↑ Powell G, Saunders M, Rigby A, Marson AG (December 2016). "Immediate-release versus controlled-release carbamazepine in the treatment of epilepsy". The Cochrane Database of Systematic Reviews. 12: CD007124. doi:10.1002/14651858.CD007124.pub5. PMC 6463840. PMID 27933615.
- ↑ Ilangaratne NB, Mannakkara NN, Bell GS, Sander JW (December 2012). "Phenobarbital: missing in action". Bulletin of the World Health Organization. 90 (12): 871–871A. doi:10.2471/BLT.12.113183. PMC 3524964. PMID 23284189.
- ↑ Shorvon, Simon; Perucca, Emilio; Engel Jr., Jerome, eds. (2009). The treatment of epilepsy (3rd ed.). Chichester, UK: Wiley-Blackwell. p. 587. ISBN 9781444316674. Archived from the original on 21 May 2016.
- 1 2 3 4 5 6 Perucca P, Gilliam FG (September 2012). "Adverse effects of antiepileptic drugs". The Lancet. Neurology. 11 (9): 792–802. doi:10.1016/S1474-4422(12)70153-9. PMID 22832500.
- 1 2 Weston J, Bromley R, Jackson CF, Adab N, Clayton-Smith J, Greenhalgh J, Hounsome J, McKay AJ, Tudur Smith C, Marson AG (November 2016). "Monotherapy treatment of epilepsy in pregnancy: congenital malformation outcomes in the child". The Cochrane Database of Systematic Reviews. 11: CD010224. doi:10.1002/14651858.CD010224.pub2. PMC 6465055. PMID 27819746.
- 1 2 Kamyar M, Varner M (June 2013). "Epilepsy in pregnancy". Clinical Obstetrics and Gynecology. 56 (2): 330–41. doi:10.1097/GRF.0b013e31828f2436. PMID 23563876.
- ↑ Lawrence S. Neinstein, ed. (2008). Adolescent health care : a practical guide (5th ed.). Philadelphia: Lippincott Williams & Wilkins. p. 335. ISBN 978-0-7817-9256-1. Archived from the original on 1 August 2020. Retrieved 15 July 2020.
- 1 2 Krucoff MO, Chan AY, Harward SC, Rahimpour S, Rolston JD, Muh C, Englot DJ (December 2017). "Rates and predictors of success and failure in repeat epilepsy surgery: A meta-analysis and systematic review". Epilepsia. 58 (12): 2133–2142. doi:10.1111/epi.13920. PMC 5716856. PMID 28994113.
- ↑ Duncan JS, Sander JW, Sisodiya SM, Walker MC (April 2006). "Adult epilepsy". Lancet. 367 (9516): 1087–1100. doi:10.1016/S0140-6736(06)68477-8. PMID 16581409.
- 1 2 3 4 5 Duncan JS (April 2007). "Epilepsy surgery". Clinical Medicine. 7 (2): 137–42. doi:10.7861/clinmedicine.7-2-137. PMC 4951827. PMID 17491501.
- ↑ Birbeck GL, Hays RD, Cui X, Vickrey BG (May 2002). "Seizure reduction and quality of life improvements in people with epilepsy". Epilepsia. 43 (5): 535–8. doi:10.1046/j.1528-1157.2002.32201.x. PMID 12027916.
- ↑ Edwards CA, Kouzani A, Lee KH, Ross EK (September 2017). "Neurostimulation Devices for the Treatment of Neurologic Disorders". Mayo Clinic Proceedings. 92 (9): 1427–1444. doi:10.1016/j.mayocp.2017.05.005. PMID 28870357.
- ↑ Panebianco M, Rigby A, Weston J, Marson AG (April 2015). "Vagus nerve stimulation for partial seizures". The Cochrane Database of Systematic Reviews (4): CD002896. doi:10.1002/14651858.CD002896.pub2. PMC 7138043. PMID 25835947.
- ↑ Maria, Bernard L., ed. (2009). Current management in child neurology (4th ed.). Hamilton, Ont.: BC Decker. p. 180. ISBN 978-1-60795-000-4. Archived from the original on 24 June 2016.
- ↑ Verrotti A, Tocco AM, Salladini C, Latini G, Chiarelli F (November 2005). "Human photosensitivity: from pathophysiology to treatment". European Journal of Neurology. 12 (11): 828–41. doi:10.1111/j.1468-1331.2005.01085.x. PMID 16241971.
- ↑ Tan G, Thornby J, Hammond DC, Strehl U, Canady B, Arnemann K, Kaiser DA (July 2009). "Meta-analysis of EEG biofeedback in treating epilepsy". Clinical EEG and Neuroscience. 40 (3): 173–9. doi:10.1177/155005940904000310. PMID 19715180.
- ↑ Arida RM, Scorza FA, Scorza CA, Cavalheiro EA (March 2009). "Is physical activity beneficial for recovery in temporal lobe epilepsy? Evidences from animal studies". Neuroscience and Biobehavioral Reviews. 33 (3): 422–31. doi:10.1016/j.neubiorev.2008.11.002. PMID 19059282.
- ↑ Arida RM, Cavalheiro EA, da Silva AC, Scorza FA (2008). "Physical activity and epilepsy: proven and predicted benefits". Sports Medicine. 38 (7): 607–15. doi:10.2165/00007256-200838070-00006. PMID 18557661.
- ↑ Di Vito L, Naldi I, Mostacci B, Licchetta L, Bisulli F, Tinuper P (June 2010). "A seizure response dog: video recording of reacting behaviour during repetitive prolonged seizures". Epileptic Disorders. 12 (2): 142–5. doi:10.1684/epd.2010.0313. PMID 20472528. Archived from the original on 6 October 2014.
- ↑ Kirton A, Winter A, Wirrell E, Snead OC (October 2008). "Seizure response dogs: evaluation of a formal training program". Epilepsy & Behavior. 13 (3): 499–504. doi:10.1016/j.yebeh.2008.05.011. PMID 18595778.
- ↑ Doherty MJ, Haltiner AM (January 2007). "Wag the dog: skepticism on seizure alert canines". Neurology. 68 (4): 309. CiteSeerX 10.1.1.1003.1543. doi:10.1212/01.wnl.0000252369.82956.a3. PMID 17242343.
- 1 2 3 Michaelis R, Tang V, Wagner JL, Modi AC, LaFrance Jr WC, Goldstein LH, Lundgren T, Reuber M (October 2017). "Psychological treatments for people with epilepsy". Cochrane Database of Systematic Reviews. 10 (10): CD012081. doi:10.1002/14651858.CD012081.pub2. PMC 6485515. PMID 29078005.
{{cite journal}}: CS1 maint: uses authors parameter (link) - ↑ Stockings E, Zagic D, Campbell G, Weier M, Hall WD, Nielsen S, Herkes GK, Farrell M, Degenhardt L (July 2018). "Evidence for cannabis and cannabinoids for epilepsy: a systematic review of controlled and observational evidence". Journal of Neurology, Neurosurgery, and Psychiatry. 89 (7): 741–753. doi:10.1136/jnnp-2017-317168. PMID 29511052.
- ↑ "Press Announcements - FDA approves first drug comprised of an active ingredient derived from marijuana to treat rare, severe forms of epilepsy". www.fda.gov. 25 June 2018. Archived from the original on 23 April 2019. Retrieved 4 October 2018.
- ↑ Cheuk DK, Wong V (May 2014). "Acupuncture for epilepsy". The Cochrane Database of Systematic Reviews. 5 (5): CD005062. doi:10.1002/14651858.CD005062.pub4. PMID 24801225.
- ↑ Ranganathan LN, Ramaratnam S (April 2005). "Vitamins for epilepsy". The Cochrane Database of Systematic Reviews (2): CD004304. doi:10.1002/14651858.CD004304.pub2. PMID 15846704.
- ↑ Panebianco M, Sridharan K, Ramaratnam S (October 2017). "Yoga for epilepsy". The Cochrane Database of Systematic Reviews. 10: CD001524. doi:10.1002/14651858.CD001524.pub3. PMC 6485327. PMID 28982217.
- 1 2 Brigo F, Igwe SC, Del Felice A (August 2016). "Melatonin as add-on treatment for epilepsy". The Cochrane Database of Systematic Reviews (8): CD006967. doi:10.1002/14651858.CD006967.pub4. PMID 27513702.
- 1 2 Kwan, Patrick (2012). Fast facts : epilepsy (5th ed.). Abingdon, Oxford, UK: Health Press. p. 10. ISBN 978-1-908541-12-3.
- 1 2 3 Hitiris N, Mohanraj R, Norrie J, Brodie MJ (May 2007). "Mortality in epilepsy". Epilepsy & Behavior. 10 (3): 363–76. doi:10.1016/j.yebeh.2007.01.005. PMID 17337248.
- 1 2 3 Shorvon, Simon; Perucca, Emilio; Engel, Jerome, eds. (2009). The treatment of epilepsy (3rd ed.). Chichester, UK: Wiley-Blackwell. p. 28. ISBN 978-1-4443-1667-4. Archived from the original on 10 June 2016.
- 1 2 Bagary M (April 2011). "Epilepsy, antiepileptic drugs and suicidality". Current Opinion in Neurology. 24 (2): 177–82. doi:10.1097/WCO.0b013e328344533e. PMID 21293270.
- ↑ Mula M, Sander JW (August 2013). "Suicide risk in people with epilepsy taking antiepileptic drugs". Bipolar Disorders. 15 (5): 622–7. doi:10.1111/bdi.12091. PMID 23755740.
- 1 2 Ryvlin P, Nashef L, Tomson T (May 2013). "Prevention of sudden unexpected death in epilepsy: a realistic goal?". Epilepsia. 54 Suppl 2: 23–8. doi:10.1111/epi.12180. PMID 23646967.
- ↑ Hirtz D, Thurman DJ, Gwinn-Hardy K, Mohamed M, Chaudhuri AR, Zalutsky R (January 2007). "How common are the "common" neurologic disorders?". Neurology. 68 (5): 326–37. doi:10.1212/01.wnl.0000252807.38124.a3. PMID 17261678.
- ↑ Espinosa-Jovel, Camilo; Toledano, Rafael; Aledo-Serrano, Ángel; García-Morales, Irene; Gil-Nagel, Antonio (2018-03-01). "Epidemiological profile of epilepsy in low income populations". Seizure - European Journal of Epilepsy. 56: 67–72. doi:10.1016/j.seizure.2018.02.002. ISSN 1059-1311. PMID 29453113. Archived from the original on 29 August 2021. Retrieved 15 July 2020.
- 1 2 Sander JW (April 2003). "The epidemiology of epilepsy revisited". Current Opinion in Neurology. 16 (2): 165–70. doi:10.1097/00019052-200304000-00008. PMID 12644744.
- 1 2 3 4 5 6 7 8 Saraceno B, Avanzini G, Lee P, eds. (2005). Atlas: Epilepsy Care in the World (PDF). World Health Organization. ISBN 978-92-4-156303-1. Archived (PDF) from the original on 25 October 2013. Retrieved 20 December 2013.
- ↑ Eadie, Mervyn J.; Bladin, Peter F. (2001). A Disease Once Sacred: A History of the Medical Understanding of Epilepsy. John Libbey Eurotext. ISBN 978-0-86196-607-3. Archived from the original on 1 August 2020. Retrieved 15 July 2020.
- ↑ "Epilepsy: An historical overview". World Health Organization. Feb 2001. Archived from the original on 30 October 2013. Retrieved 27 December 2013.
- ↑ "Epilepsy: historical overview". World Health Organization. Archived from the original on 20 January 2011. Retrieved 2011-03-20.
- 1 2 Temkin, Owsei (1994-03-01). The Falling Sickness: A History of Epilepsy from the Greeks to the Beginnings of Modern Neurology. JHU Press. p. Section 1. ISBN 9781421400532. Archived from the original on 1 August 2020. Retrieved 15 July 2020.
- ↑ Stol, Marten (1993). Epilepsy in Babylonia. BRILL. p. 143. ISBN 978-9072371638. Archived from the original on 1 August 2020. Retrieved 15 July 2020.
- ↑ Harding, Graham F. A.; Jeavons, Peter M. (1994). Photosensitive Epilepsy. Cambridge University Press. p. 2. ISBN 9781898683025. Archived from the original on 1 August 2020. Retrieved 15 July 2020.
- 1 2 Jilek-Aall L (March 1999). "Morbus sacer in Africa: some religious aspects of epilepsy in traditional cultures". Epilepsia. 40 (3): 382–6. doi:10.1111/j.1528-1157.1999.tb00723.x. PMID 10080524.
- ↑ Illes, Judika (2011). Encyclopedia of Mystics, Saints & Sages. HarperCollins. p. 1238. ISBN 978-0-06-209854-2. Archived from the original on 11 January 2014.
Saint Valentine is invoked for healing as well as love. He protects against fainting and is requested to heal epilepsy and other seizure disorders. In northern Italy, epilepsy was once traditionally known as Saint Valentine's Malady.
- ↑ Caravati, E. Martin (2004). Medical toxicology (3rd ed.). Philadelphia [u.a.]: Lippincott Williams & Wilkins. p. 789. ISBN 978-0-7817-2845-4. Archived from the original on 1 August 2020. Retrieved 15 July 2020.
- 1 2 de Boer HM (December 2010). "Epilepsy stigma: moving from a global problem to global solutions". Seizure. 19 (10): 630–6. doi:10.1016/j.seizure.2010.10.017. PMID 21075013.
- ↑ Martindale JL, Goldstein JN, Pallin DJ (February 2011). "Emergency department seizure epidemiology". Emergency Medicine Clinics of North America. 29 (1): 15–27. doi:10.1016/j.emc.2010.08.002. PMID 21109099.
- 1 2 3 4 Engel J, Pedley TA, eds. (2008). Epilepsy : a comprehensive textbook (2nd ed.). Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins. p. 2279. ISBN 978-0-7817-5777-5. Archived from the original on 1 August 2020. Retrieved 15 July 2020.
- ↑ Bor, Robert (2012). Aviation Mental Health: Psychological Implications for Air Transportation. Ashgate Publishing. p. 148. ISBN 978-1-4094-8491-2. Archived from the original on 1 August 2020. Retrieved 15 July 2020.
- 1 2 "Seizure Disorders". Transport Canada. Government of Canada. Archived from the original on 30 December 2013. Retrieved 29 December 2013.
- ↑ Wilner, Andrew N. (2008). Epilepsy 199 answers : a doctor responds to his patients' questions (3rd ed.). New York: Demos Health. p. 52. ISBN 978-1-934559-96-3. Archived from the original on 17 May 2016.
- ↑ "Guide for Aviation Medical Examiners". Federal Aviation Administration. Archived from the original on 17 October 2013. Retrieved 29 December 2013.
- 1 2 "National PPL (NPPL) Medical Requirements". Civil Aviation Authority. Archived from the original on 16 October 2013. Retrieved 29 December 2013.
- ↑ Drivers Medical Group (2013). "For Medical Practitioners: At a glance Guide to the current Medical Standards of Fitness to Drive" (PDF). p. 8. Archived (PDF) from the original on 30 December 2013. Retrieved 29 December 2013.
- ↑ "Epilepsy Foundation of America - EFA". Healthfinder.gov. US Department of Health and Human Services. 28 April 2011. Archived from the original on 16 July 2014. Retrieved 28 July 2014.
- ↑ Engel J, Pedley TA, eds. (2008). Epilepsy: a comprehensive textbook (2nd ed.). Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins. p. 2245. ISBN 9780781757775. Archived from the original on 1 August 2020. Retrieved 15 July 2020.
- ↑ Aleem, MA (February 2015). "Letter: World Epilepsy Day". Epilepsia. 56 (2): 168. doi:10.1111/epi.12814. PMID 25404065.
- ↑ Perucca, Emilio (February 2015). "Commentary: Why an International Epilepsy Day?". Epilepsia. 56 (2): 170–171. doi:10.1111/epi.12813. PMID 25403985.
- 1 2 Carney PR, Myers S, Geyer JD (December 2011). "Seizure prediction: methods". Epilepsy & Behavior. 22 Suppl 1: S94–101. doi:10.1016/j.yebeh.2011.09.001. PMC 3233702. PMID 22078526.
- ↑ Engel J, ed. (2008). Epilepsy: a comprehensive textbook (2nd ed.). Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins. p. 426. ISBN 9780781757775. Archived from the original on 1 August 2020. Retrieved 15 July 2020.
- ↑ Walker MC, Schorge S, Kullmann DM, Wykes RC, Heeroma JH, Mantoan L (September 2013). "Gene therapy in status epilepticus" (PDF). Epilepsia. 54 Suppl 6: 43–5. doi:10.1111/epi.12275. PMID 24001071. Archived (PDF) from the original on 23 July 2018. Retrieved 15 July 2020.
- ↑ Walker L, Pirmohamed M, Marson AG (June 2013). "Immunomodulatory interventions for focal epilepsy syndromes". The Cochrane Database of Systematic Reviews. 6 (6): CD009945. doi:10.1002/14651858.CD009945.pub2. PMID 23803963.
- ↑ Quigg M, Rolston J, Barbaro NM (January 2012). "Radiosurgery for epilepsy: clinical experience and potential antiepileptic mechanisms". Epilepsia. 53 (1): 7–15. doi:10.1111/j.1528-1167.2011.03339.x. PMC 3519388. PMID 22191545.
- 1 2 Thomas WB (January 2010). "Idiopathic epilepsy in dogs and cats". The Veterinary Clinics of North America. Small Animal Practice. 40 (1): 161–79. doi:10.1016/j.cvsm.2009.09.004. PMID 19942062.
- ↑ Rundfeldt C, Löscher W (January 2014). "The pharmacology of imepitoin: the first partial benzodiazepine receptor agonist developed for the treatment of epilepsy". CNS Drugs. 28 (1): 29–43. doi:10.1007/s40263-013-0129-z. PMID 24357084.
- ↑ van der Ree M, Wijnberg I (2012). "A review on epilepsy in the horse and the potential of Ambulatory EEG as a diagnostic tool". The Veterinary Quarterly. 32 (3–4): 159–67. doi:10.1080/01652176.2012.744496. PMID 23163553.
Further reading
- World Health Organization, Department of Mental Health and Substance Abuse, Programme for Neurological Diseases and Neuroscience; Global Campaign against Epilepsy; International League against Epilepsy (2005). Atlas, epilepsy care in the world, 2005 (PDF). Geneva: Programme for Neurological Diseases and Neuroscience, Department of Mental Health and Substance Abuse, World Health Organization. ISBN 978-92-4-156303-1. Archived (PDF) from the original on 25 October 2013. Retrieved 15 July 2020.
{{cite book}}: CS1 maint: multiple names: authors list (link) - Scheffer IE, Berkovic S, Capovilla G, Connolly MB, French J, Guilhoto L, Hirsch E, Jain S, Mathern GW, Moshé SL, Nordli DR, Perucca E, Tomson T, Wiebe S, Zhang YH, Zuberi SM (April 2017). "ILAE classification of the epilepsies: Position paper of the ILAE Commission for Classification and Terminology". Epilepsia. 58 (4): 512–521. doi:10.1111/epi.13709. PMC 5386840. PMID 28276062.
External links
| Classification | |
|---|---|
| External resources |
- Epilepsy at Curlie
- World Health Organization fact sheet Archived 11 March 2016 at the Wayback Machine