MALT lymphoma
| MALT lymphoma | |
|---|---|
 | |
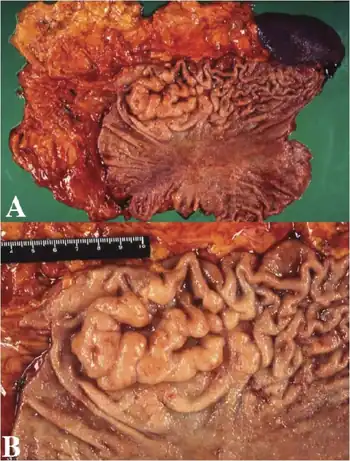
| Endoscopic image of gastric MALT lymphoma taken in body of stomach in patient who presented with upper GI hemorrhage. Appearance is similar to gastric ulcer with adherent clot. | |
MALT lymphoma (MALToma) is a form of lymphoma involving the mucosa-associated lymphoid tissue (MALT), frequently of the stomach, but virtually any mucosal site can be afflicted. It is a cancer originating from B cells in the marginal zone of the MALT, and is also called extranodal marginal zone B cell lymphoma.
Signs and symptoms
Associations
Gastric MALT lymphoma is frequently associated (72–98%) with chronic inflammation as a result of the presence of Helicobacter pylori,[1] potentially involving chronic inflammation, or the action of H. pylori virulence factors such as CagA.[2]
The initial diagnosis is made by biopsy of suspicious lesions on esophagogastroduodenoscopy (EGD, upper endoscopy). Simultaneous tests for H. pylori are also done to detect the presence of this microbe.[3]
In other sites, chronic immune stimulation is also suspected in the pathogenesis (e.g. association between chronic autoimmune diseases such as Sjögren's syndrome and Hashimoto's thyroiditis, and MALT lymphoma of the salivary gland and the thyroid).[4]
Diagnosis
MALT lymphoma is an often multifocal disease in the organ of origin and is frequently macroscopically indistinguishable from other disease processes in the GI tract. Endoscopy is key to diagnosing MALT lymphoma, with multiple biopsies of the visible lesions required, as well as samples of macroscopically normal tissue, termed gastric mapping. Histologically, there is expansion of the marginal zone compartment with development of sheets of neoplastic small lymphoid cells.[5] The morphology of the neoplastic cells is variable with small mature lymphocytes, cells resembling centrocytes (centrocyte like cells), or marginal zone/monocytoid B cells. Plasmacytoid or plasmacytic differentiation is frequent. Lymphoid follicles are ubiquitous to MALT lymphoma but may be indistinct as they are often overrun or colonized by the neoplastic cells. Large transformed B cells are presently scattered among the small cell population. If these large cells are present in clusters or sheets, a diagnosis of associated large B-cell lymphoma should be considered. A characteristic feature of MALT lymphoma is the presence of neoplastic cells within epithelial structures with associated destruction of the glandular architecture to form lymphoepithelial lesions.[6]
MALT lymphoma may be difficult to distinguish from reactive infiltrates, and in some cases, multiple endoscopies are required before a confident diagnosis is reached. The Wotherspoon score, which grades the presence of histological features associated with MALT lymphoma, is useful in expressing confidence in diagnosis at presentation. Immunohistochemistry can be used to help distinguish MALT lymphoma from other small B-cell NHLs. B-cell-associated antigens such as CD19, CD20, CD22, and CD79a are usually expressed. In contrast to small lymphocytic lymphoma and MCL, staining for CD5 is usually negative, and these lymphomas can be further distinguished with CD23 (positive in small lymphocytic lymphoma) and CyclinD1 (positive in MCL).[7]
Treatment
Owing to the causal relationship between H. pylori infection and MALT lymphoma, identification of the infection is imperative. Histological examination of GI biopsies yields a sensitivity of 95% with five biopsies,[8] but these should be from sites uninvolved by lymphoma and the identification of the organism may be compromised by areas of extensive intestinal metaplasia. As proton-pump inhibition can suppress infection, any treatment with this class of drug should be ceased 2 weeks prior to biopsy retrieval. Serology should be performed if histology is negative, to detect suppressed or recently treated infections.[9] Following the recognition of the association of gastric MALT lymphoma with H. pylori infection, it was established that early-stage gastric disease could be cured by H. pylori eradication, which is now the mainstay of therapy. Fifty to 95% of cases achieve complete response (CR) with H. pylori treatment.[10][11]
A t(11;18)(q21;q21) chromosomal translocation, giving rise to an API2-MLT fusion gene,[12] is predictive of poor response to eradication therapy.[13]
Radiotherapy
Radiotherapy is a valid first option for MALT lymphoma. It provides local control and potential cure in localized gastric stage IE and II 1E disease with 5-year EFS of 85-100% reported in retrospective studies.[14][15] However, the irradiation field is potentially large as it must include the whole stomach, which can vary greatly in size and shape. Irradiation techniques have improved considerably in the last 20 years, including treating the patient in a fasting state, decreasing the irradiated field and required dose. The moderate dose of 30 Gray (Gy) of involved-field radiotherapy administered in 15 fractions (doses) can be associated with tolerable toxicity and excellent outcomes. Hence, radiotherapy is the preferred approach for local disease where antibiotic therapy has failed, or is not indicated. Evidence also suggests that radiotherapy can be utilized to control localized relapses outside the original radiation field.[16]
Chemotherapy
MALT lymphoma is exquisitely immunotherapy sensitive. Chemotherapy is reserved for those uncommon patients with disseminated disease at presentation or lack of response to local treatment. Rituximab, the anti-CD20 chimeric antibody, is a key component of therapy. Responses vary from 55% to 77% with monotherapy and 100% in combination with chemotherapy.[17][18] Oral alkylating agents such as cyclophosphamide or chlorambucil have been administered for a median duration of 12 months with high rates of disease control (CR up to 75%) but appear not to be active in t(11;18) disease.[19] The purine nucleoside analogs fludarabine and cladribine also demonstrate activity,[20] the latter conferring a CR rate of 84% (100% in those with gastric primaries) in a small study.[21] A pivotal study of rituximab plus chlorambucil compared with chlorambucil alone (IELSG-19 study, n = 227) demonstrated a significantly higher CR rate (78% vs. 65%; p = 0.017) and 5-year EFS (68% vs. 50%; p = 0.024) over chlorambucil alone. However, 5-year OS was not improved (88% in both arms). First-line treatment of choice is generally rituximab in combination with single alkylating agents or fludarabine, or a combination of all three drugs. The final results of this study, including the later addition of a rituximab-alone arm, are pending.[22]
Two other genetic alterations are known:
- t(1;14)(p22;q32), which deregulates BCL10, at the locus 1p22.
- t(14;18)(q32;q21), which deregulates MALT1, at the locus 18q21.
These seem to turn on the same pathway as API2-MLT (i.e., that of NF-κB). They both act upon IGH,[23] which is at the locus 14q32.
Epidemiology
Of all cancers involving the same class of blood cell, 8% of cases are MALT lymphomas.[24]
See also
References
- ↑ Parsonnet J, Hansen S, Rodriguez L, Gelb A, Warnke R, Jellum E, Orentreich N, Vogelman J, Friedman G (1994). "Helicobacter pylori infection and gastric lymphoma". N Engl J Med. 330 (18): 1267–71. doi:10.1056/NEJM199405053301803. PMID 8145781.
- ↑ Hatakeyama, M.; Higashi, H. (2005). "Helicobacter pylori CagA: a new paradigm for bacterial carcinogenesis". Cancer Science. 96 (12): 835–843. doi:10.1111/j.1349-7006.2005.00130.x. PMID 16367902.
- ↑ "MALT Lymphoma". The Lecturio Medical Concept Library. Archived from the original on 10 August 2021. Retrieved 10 August 2021.
- ↑ "MALT Lymphoma". The Lecturio Medical Concept Library. Archived from the original on 10 August 2021. Retrieved 10 August 2021.
- ↑ Taal BG, Boot H, van Heerde P, de Jong D, Hart AA, Burgers JM (October 1996). "Primary non-Hodgkin lymphoma of the stomach: endoscopic pattern and prognosis in low versus high grade malignancy in relation to the MALT concept". Gut. 39 (4): 556–61. doi:10.1136/gut.39.4.556. PMC 1383269. PMID 8944565.
- ↑ Jankowski J, Hawk E, eds. (2012). Handbook of Gastrointestinal Cancer (2 ed.). Chicester: John Wiley and Sons Ltd. pp. 243–244. ISBN 978-0-470-65624-2.
- ↑ Wotherspoon, AC; Doglioni, C; Diss, TC; Pan, L; Moschini, A; de Boni, M; Isaacson, PG (4 September 1993). "Regression of primary low-grade B-cell gastric lymphoma of mucosa-associated lymphoid tissue type after eradication of Helicobacter pylori". Lancet. 342 (8871): 575–7. doi:10.1016/0140-6736(93)91409-f. PMID 8102719. S2CID 9531600.
- ↑ Bayerdörffer E, Oertel H, Lehn N, Kasper G, Mannes GA, Sauerbruch T, Stolte M (August 1989). "Topographic association between active gastritis and Campylobacter pylori colonisation". J. Clin. Pathol. 42 (8): 834–9. doi:10.1136/jcp.42.8.834. PMC 1142061. PMID 2768523.
- ↑ Park, Jeong Bae (2014). "infection in gastric mucosa-associated lymphoid tissue lymphoma". World Journal of Gastroenterology. 20 (11): 2751–9. doi:10.3748/wjg.v20.i11.2751. PMC 3961970. PMID 24659867.
- ↑ Fischbach, W; Goebeler, M E; Ruskone-Fourmestraux, A; Wundisch, T; Neubauer, A; Raderer, M; Savio, A (1 December 2007). "Most patients with minimal histological residuals of gastric MALT lymphoma after successful eradication of Helicobacter pylori can be managed safely by a watch and wait strategy: experience from a large international series". Gut. 56 (12): 1685–1687. doi:10.1136/gut.2006.096420. PMC 2095715. PMID 17639089.
- ↑ Sarah, Silverman. "MALT lymphoma Diagnosis, Staging, Treatment". pylori.org. UEG. Archived from the original on 2015-01-05. Retrieved 2022-01-22.
- ↑ Noels H, van Loo G, Hagens S, et al. (April 2007). "A Novel TRAF6 binding site in MALT1 defines distinct mechanisms of NF-kappaB activation by API2middle dotMALT1 fusions". J. Biol. Chem. 282 (14): 10180–9. doi:10.1074/jbc.M611038200. PMID 17287209. Archived from the original on 2019-12-14. Retrieved 2022-01-22.
- ↑ Liu H, Ruskon-Fourmestraux A, Lavergne-Slove A, Ye H, Molina T, Bouhnik Y, Hamoudi RA, Diss TC, Dogan A, Megraud F, Rambaud JC, Du MQ, Isaacson PG (January 2001). "Resistance of t(11;18) positive gastric mucosa-associated lymphoid tissue lymphoma to Helicobacter pylori eradication therapy". Lancet. 357 (9249): 39–40. doi:10.1016/S0140-6736(00)03571-6. PMID 11197361. S2CID 22237525.
- ↑ Tomita N, Kodaira T, Tachibana H, Nakamura T, Mizoguchi N, Takada A (February 2009). "Favorable outcomes of radiotherapy for early-stage mucosa-associated lymphoid tissue lymphoma". Radiother Oncol. 90 (2): 231–5. doi:10.1016/j.radonc.2008.12.004. PMID 19135751.
- ↑ Schechter NR, Portlock CS, Yahalom J (May 1998). "Treatment of mucosa-associated lymphoid tissue lymphoma of the stomach with radiation alone". J. Clin. Oncol. 16 (5): 1916–21. doi:10.1200/JCO.1998.16.5.1916. PMID 9586910.
- ↑ Avilés A, Nambo MJ, Neri N, Talavera A, Cleto S (2005). "Mucosa-associated lymphoid tissue (MALT) lymphoma of the stomach: results of a controlled clinical trial". Med. Oncol. 22 (1): 57–62. doi:10.1385/MO:22:1:057. PMID 15750197. S2CID 29541664.
- ↑ Conconi A, Martinelli G, Thiéblemont C, Ferreri AJ, Devizzi L, Peccatori F, et al. (October 2003). "Clinical activity of rituximab in extranodal marginal zone B-cell lymphoma of MALT type". Blood. 102 (8): 2741–5. doi:10.1182/blood-2002-11-3496. PMID 12842999.
- ↑ Martinelli G, Laszlo D, Ferreri AJ, Pruneri G, Ponzoni M, Conconi A, et al. (March 2005). "Clinical activity of rituximab in gastric marginal zone non-Hodgkin's lymphoma resistant to or not eligible for anti-Helicobacter pylori therapy". J. Clin. Oncol. 23 (9): 1979–83. doi:10.1200/JCO.2005.08.128. PMID 15668468.
- ↑ Lévy M, Copie-Bergman C, Gameiro C, Chaumette MT, Delfau-Larue MH, Haioun C, et al. (August 2005). "Prognostic value of translocation t(11;18) in tumoral response of low-grade gastric lymphoma of mucosa-associated lymphoid tissue type to oral chemotherapy". J. Clin. Oncol. 23 (22): 5061–6. doi:10.1200/JCO.2005.05.660. PMID 16051953.
- ↑ Zinzani PL, Stefoni V, Musuraca G, Tani M, Alinari L, Gabriele A, et al. (May 2004). "Fludarabine-containing chemotherapy as frontline treatment of nongastrointestinal mucosa-associated lymphoid tissue lymphoma". Cancer. 100 (10): 2190–4. doi:10.1002/cncr.20237. PMID 15139063. S2CID 25251522.
- ↑ Jäger G, Neumeister P, Quehenberger F, Wöhrer S, Linkesch W, Raderer M (November 2006). "Prolonged clinical remission in patients with extranodal marginal zone B-cell lymphoma of the mucosa-associated lymphoid tissue type treated with cladribine: 6 year follow-up of a phase II trial". Ann. Oncol. 17 (11): 1722–3. doi:10.1093/annonc/mdl126. PMID 16766585.
- ↑ Zucca E, Conconi A, Laszlo D, López-Guillermo A, Bouabdallah R, Coiffier B, et al. (February 2013). "Addition of rituximab to chlorambucil produces superior event-free survival in the treatment of patients with extranodal marginal-zone B-cell lymphoma: 5-year analysis of the IELSG-19 Randomized Study". J. Clin. Oncol. 31 (5): 565–72. doi:10.1200/JCO.2011.40.6272. PMID 23295789.
- ↑ Ye H, Gong L, Liu H, Hamoudi RA, Shirali S, Ho L, et al. (February 2005). "MALT lymphoma with t(14;18)(q32;q21)/IGH-MALT1 is characterized by strong cytoplasmic MALT1 and BCL10 expression". J. Pathol. 205 (3): 293–301. doi:10.1002/path.1715. PMID 15682443. S2CID 41038826.
- ↑ Turgeon, Mary Louise (2005). Clinical hematology: theory and procedures. Hagerstown, MD: Lippincott Williams & Wilkins. p. 283. ISBN 0-7817-5007-5.
Frequency of lymphoid neoplasms. (Source: Modified from WHO Blue Book on Tumour of Hematopoietic and Lymphoid Tissues. 2001, p. 2001.)
External links
| Classification |
|---|