Osteopetrosis
| Adult-onset osteopetrosis (Albers-Schönberg Disease) | |
|---|---|
 | |
| X-ray of the pelvis of a patient with osteopetrosis, adult onset form (Albers-Schönberg disease). Note the dense appearance. | |
Osteopetrosis, literally "stone bone", also known as marble bone disease or Albers-Schönberg disease, is an extremely rare inherited disorder whereby the bones harden, becoming denser, in contrast to more prevalent conditions like osteoporosis, in which the bones become less dense and more brittle, or osteomalacia, in which the bones soften. Osteopetrosis can cause bones to dissolve and break.[1]
It is one of the hereditary causes of osteosclerosis.[2] It is considered to be the prototype of osteosclerosing dysplasias. The cause of the disease is understood to be malfunctioning osteoclasts and their inability to resorb bone. Although human osteopetrosis is a heterogeneous disorder encompassing different molecular lesions and a range of clinical features, all forms share a single pathogenic nexus in the osteoclast. The exact molecular defects or location of the mutations taking place are unknown.[3] Osteopetrosis was first described in 1903, by German radiologist Albers-Schönberg.
Signs and symptoms

Despite this excess bone formation, people with osteopetrosis tend to have bones that are more brittle than normal. Mild osteopetrosis may cause no symptoms, and present no problems.[4]
However, serious forms can result in the following:[4]
- Stunted growth, deformity, and increased likelihood of fractures
- Patients suffer anemia, recurrent infections, and hepatosplenomegaly due to bone expansion leading to bone marrow narrowing and extramedullary hematopoiesis
- It can also result in blindness, facial paralysis, and deafness, due to the increased pressure put on the nerves by the extra bone
- Abnormal cortical bone morphology
- Abnormal form of the vertebral bodies
- Abnormality of temperature regulation
- Abnormality of the ribs
- Abnormality of vertebral epiphysis morphology
- Bone pain
- Cranial nerve paralysis
- Craniosynostosis
- Hearing impairment
- Hypocalcemia
| Condition | Calcium | Phosphate | Alkaline phosphatase | Parathyroid hormone | Comments |
|---|---|---|---|---|---|
| Osteopenia | unaffected | unaffected | normal | unaffected | decreased bone mass |
| Osteopetrosis | unaffected | unaffected | elevated | unaffected | thick dense bones also known as marble bone |
| Osteomalacia and rickets | decreased | decreased | elevated | elevated | soft bones |
| Osteitis fibrosa cystica | elevated | decreased | elevated | elevated | brown tumors |
| Paget's disease of bone | unaffected | unaffected | variable (depending on stage of disease) | unaffected | abnormal bone architecture |
Malignant infantile osteopetrosis
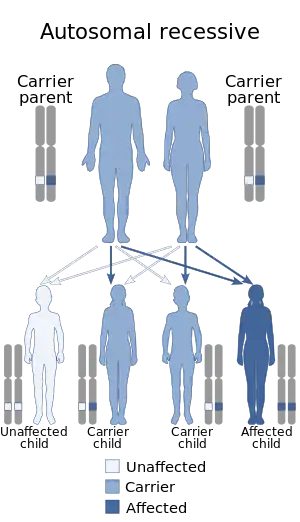
Autosomal recessive osteopetrosis (ARO), also known as malignant infantile osteopetrosis or infantile malignant osteopetrosis (IMO), is a rare type of skeletal dysplasia characterized by a distinct radiographic pattern of overall increased density of the bones with fundamental involvement of the medullary portion. Infantile osteopetrosis typically manifests in infancy. Diagnosis is principally based on clinical and radiographic evaluation, confirmed by gene analysis where applicable.[5] As a result of medullary canal obliteration and bony expansion, grave pancytopenia, cranial nerve compression, and pathologic fractures may ensue. The prognosis is poor if untreated. The classic radiographic features include endobone or "bone-within-bone" appearance in the spine, pelvis and proximal femora, upper limbs, and short tubular bones of the hand. Additionally, there is the Erlenmeyer flask deformity type 2 which is characterized by the absence of normal diaphysial metaphysical modeling of the distal femora with abnormal radiographic appearance of trabecular bone and alternating radiolucent metaphyseal bands.[5]
The precise and early diagnosis of infantile osteopetrosis is important for management of complications, genetic counselling, and timely institution of appropriate treatment, namely hematopoietic stem cell transplantation (HSCT), which offers a satisfactory treatment modality for a considerable percentage of infantile osteopetrosis.[6] Amelioration of radiographic bone lesions after HSCT in infantile osteopetrosis has been proposed as an important indicator of success of the therapy. A few publications with limited study participants have demonstrated the resolution of skeletal radiographic pathology following HSCT.[7][8]
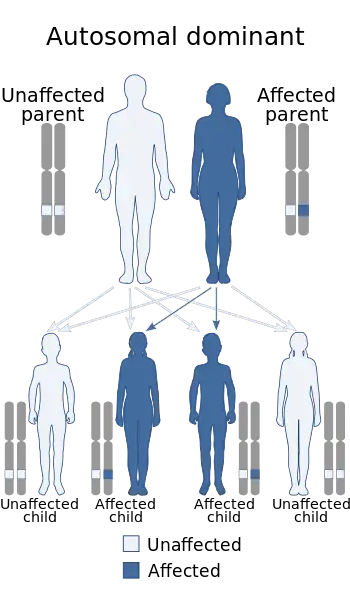
Adult osteopetrosis
Autosomal dominant osteopetrosis (ADO) is also known as Albers-Schonberg disease. Most do not know they have this disorder because most individuals do not show any symptoms. However, the ones that do show symptoms will typically have a curvature of the spine (scoliosis), and multiple bone fractures. There are two types of adult osteopetrosis based on the basis of radiographic, biochemical, and clinical features.
| Characteristic | Type I | Type II |
|---|---|---|
| Skull Sclerosis | Marked sclerosis mainly of the vault | Sclerosis mainly of the base |
| Spine | Does not show signs of sclerosis | Shows the sandwich appearance[9] |
| Pelvis | No endobones | Shows endobones in the pelvis |
| Risk of Fracture | Low | High |
| Serum Acid Phosphate | Normal | Very high |
Many patients will have bone pains. The defects are very common and include neuropathies due to cranial nerve entrapment, osteoarthritis, and carpal tunnel syndrome. About 40% of patients will experience recurrent fractures of their bones. 10% of patients will have osteomyelitis of the mandible.
Causes
The various types of osteopetrosis are caused by genetic changes (mutations) in one of at least ten genes. There is nothing a parent can do before, during or after a pregnancy to cause osteopetrosis in a child.[4]
The genes associated with osteopetrosis are involved in the development and/or function of osteoclasts, cells that break down bone tissue when old bone is being replaced by new bone (bone remodeling). This process is necessary to keep bones strong and healthy. Mutations in these genes can lead to abnormal osteoclasts, or having too few osteoclasts. If this happens, old bone cannot be broken down as new bone is formed, so bones become too dense and prone to breaking.[4]
- Mutations in the CLCN7 gene cause most cases of autosomal dominant osteopetrosis, 10-15% of cases of autosomal recessive osteopetrosis (the most severe form), and all known cases of intermediate autosomal osteopetrosis.
- Mutations in the TCIRG1 gene cause about 50% of cases of autosomal recessive osteopetrosis.
- Mutations in the IKBKG gene cause X-linked osteopetrosis.
- Mutations in other genes are less common causes of osteopetrosis.
- In about 30% percent of affected people, the cause is unknown.
Normally, bone growth is a balance between osteoblasts (cells that create bone tissue) and osteoclasts (cells that destroy bone tissue). Sufferers of osteopetrosis have a deficiency of osteoclasts, meaning too little bone is being resorbed, resulting in too much bone being created.
Gene variation
| Name | OMIM | Gene |
|---|---|---|
| OPTA1 | 607634 | LRP5 receptor |
| OPTA2 | 166600 | CLCN7 chloride channel |
| OPTB1 | 259700 | TCIRG1 ATPase |
| OPTB2 | 259710 | RANKL |
| OPTB3 | 259730 | CA2 (renal tubular acidosis) |
| OPTB4 | 611490 | CLCN7 chloride channel |
| OPTB5 | 259720 | OSTM1 ubiquitin ligase |
| OPTB6 | 611497 | PLEKHM1 adapter protein |
| OPTB7 | 612301 | TNFRSF11A (RANK receptor) |
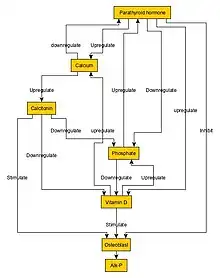
Mechanisms
Normal bone growth is achieved by a balance between bone formation by osteoblasts and bone resorption (breakdown of bone matrix) by osteoclasts.[10] In osteopetrosis, the number of osteoclasts may be reduced, normal, or increased. Most importantly, osteoclast dysfunction mediates the pathogenesis of this disease.[11]
Osteopetrosis is caused by underlying mutations that interfere with the acidification of the osteoclast resorption pit, for example due to a deficiency of the carbonic anhydrase enzyme encoded by the CA2 gene.[12] Carbonic anhydrase is required by osteoclasts for proton production. Without this enzyme hydrogen ion pumping is inhibited and bone resorption by osteoclasts is defective, as an acidic environment is needed to dissociate calcium hydroxyapatite from the bone matrix. As bone resorption fails while bone formation continues, excessive bone is formed.[13]
Mutations in at least nine genes cause the various types of osteopetrosis. Mutations in the CLCN7 gene are responsible for about 75 percent of cases of autosomal dominant osteopetrosis, 10 to 15 percent of cases of autosomal recessive osteopetrosis, and all known cases of intermediate autosomal osteopetrosis. TCIRG1 gene mutations cause about 50 percent of cases of autosomal recessive osteopetrosis. Mutations in other genes are less common causes of autosomal dominant and autosomal recessive forms of the disorder. The X-linked type of osteopetrosis, OL-EDA-ID, results from mutations in the IKBKG gene. In about 30 percent of all cases of osteopetrosis, the cause of the condition is unknown.[14]
The genes associated with osteopetrosis are involved in the formation, development, and function of specialized cells called osteoclasts. These cells break down bone tissue during bone remodeling, a normal process in which old bone is removed and new bone is created to replace it. Bones are constantly being remodeled, and the process is carefully controlled to ensure that bones stay strong and healthy.[14]
Mutations in any of the genes associated with osteopetrosis lead to abnormal or missing osteoclasts. Without functional osteoclasts, old bone is not broken down as new bone is formed. As a result, bones throughout the skeleton become unusually dense. The bones are also structurally abnormal, making them prone to fracture. These problems with bone remodeling underlie all of the major features of osteopetrosis.[14]
Diagnosis

The differential diagnosis of osteopetrosis includes other disorders that produce osteosclerosis. They constitute a wide array of disorders with clinically and radiologically diverse manifestations. Among the differential diagnosis are hereditary ostoesclerosing dysplasias such as; neuropathic infantile osteopetrosis, infantile osteopetrosis with renal tubular acidosis, infantile osteopetrosis with immunodeficiency, infantile osteopetrosis with leukocyte adhesion deficiency syndrome (LAD-III), pyknodysostosis (osteopetrosis acro-osteolytica), osteopoikilosis (Buschke–Ollendorff syndrome), osteopathia striata with cranial sclerosis, mixed sclerosing skeletal dysplasias, progressive diaphyseal dysplasia (Camurati–Engelmann disease), SOST-related sclerosing skeletal dysplasias.[5] Besides, the differential diagnosis includes acquired conditions that induce osteosclerosis such as osteosclerotic metastasis notably carcinomas of the prostate gland and breast, Paget's disease of bone, myelofibrosis (primary disorder or secondary to intoxication or malignancy), Erdheim-Chester disease, osteosclerosing types of osteomyelitis, sickle cell disease, hypervitaminosis D, and hypoparathyroidism.[15]
Treatment
It was the first genetic disease treated with hematopoietic stem cell transplantation (osteoclasts are derived from hematopoietic precursors). There is no cure, although curative therapy with bone marrow transplantion is being investigated in clinical trials. It is believed the healthy marrow will provide the sufferer with cells from which osteoclasts will develop.[4] If complications occur in children, patients can be treated with vitamin D. Gamma interferon has also been shown to be effective, and it can be associated to vitamin D. Erythropoetin has been used to treat any associated anemia. Corticosteroids may alleviate both the anemia and stimulate bone resorption. Fractures and osteomyelitis can be treated as usual.[4] Treatment for osteopetrosis depends on the specific symptoms present and the severity in each person. Therefore, treatment options must be evaluated on an individual basis. Nutritional support is important to improve growth and it also enhances responsiveness to other treatment options. A calcium-deficient diet has been beneficial for some affected people.[4]
Treatment is necessary for the infantile form:[4]
- Vitamin D (calcitriol) appears to stimulate dormant osteoclasts, which stimulates bone resorption
- Gamma interferon can have long-term benefits. It improves white blood cell function (leading to fewer infections), decreases bone volume, and increases bone marrow volume.
- Erythropoietin can be used for anemia, and corticosteroids can be used for anemia and to stimulate bone resorption.
Bone marrow transplantation (BMT) improves some cases of severe, infantile osteopetrosis associated with bone marrow failure, and offers the best chance of longer-term survival for individuals with this type.[4]
In pediatric (childhood) osteopetrosis, surgery is sometimes needed because of fractures. Adult osteopetrosis typically does not require treatment, but complications of the condition may require intervention. Surgery may be needed for aesthetic or functional reasons (such as multiple fractures, deformity, and loss of function), or for severe degenerative joint disease.[4]
Prognosis
The long-term-outlook for people with osteopetrosis depends on the subtype and the severity of the condition in each person. The severe infantile forms of osteopetrosis are associated with shortened life expectancy, with most untreated children not surviving past their first decade. Bone marrow transplantation seems to have cured some infants with early-onset disease. However, the long-term prognosis after transplantation is unknown. For those with onset in childhood or adolescence, the effect of the condition depends on the specific symptoms (including how fragile the bones are and how much pain is present). Life expectancy in the adult-onset forms is normal.[16]
Prevalence
Approximately eight to 40 children are born in the United States each year with the malignant infantile type of osteopetrosis. One in every 100,000 to 500,000 individuals is born with this form of osteopetrosis. Higher rates have been found in Denmark and Costa Rica. Males and females are affected in equal numbers.[17]
The adult type of osteopetrosis affects about 1,250 individuals in the United States. One in every 200,000 individuals is affected by the adult type of osteopetrosis. Higher rates have been found in Brazil. Males and females are affected in equal numbers.[17]
Osteopetrosis affects one newborn out of every 20,000 to 250,000[18] worldwide, but the odds are much higher in the Russian region of Chuvashia (1 of every 3,500–4,000 newborns) due to genetic traits of the Chuvash people.[19][20]
Recent research
Recent research demonstrated that the systematic administration of RANKL for one month to Rankl(-/-) mice, which closely resemble the human disease, significantly improved the bone phenotype and has beneficial effects on bone marrow, spleen and thymus; major adverse effects arise only when mice are clearly overtreated. Overall, it provided evidence that the pharmacological administration of RANKL represents the appropriate treatment option for RANKL-deficient ARO patients, to be validated in a pilot clinical trial.[21]
Interferon gamma-1b is FDA-approved to delay the time to disease progression in patients with severe, malignant osteopetrosis.[22]
Notable cases
- Laurel Burch[23]
- Lil Bub
References
- ↑ "Marble Bone Disease: A Review of Osteopetrosis and Its Oral Health Implications for Dentists". Cda-adc.ca. Archived from the original on 2013-10-18. Retrieved 2013-10-17.
- ↑ Lam DK, Sándor GK, Holmes HI, Carmichael RP, Clokie CM (2007). "Marble bone disease: a review of osteopetrosis and its oral health implications for dentists". J Can Dent Assoc. 73 (9): 839–43. PMID 18028760. Archived from the original on 2013-10-18. Retrieved 2021-12-27.
- ↑ Stark, Zornitza; Savarirayan, Ravi (2009-02-20). "Osteopetrosis". Orphanet Journal of Rare Diseases. 4: 5. doi:10.1186/1750-1172-4-5. ISSN 1750-1172. PMC 2654865. PMID 19232111.
- 1 2 3 4 5 6 7 8 9 10 "Albers-Schonberg disease — CheckOrphan". www.checkorphan.org. Archived from the original on 2017-12-13. Retrieved 2017-12-13.
- 1 2 3 Elsobky TA, Elsobky E, Sadek I, Elsayed SM, Khattab MF (2016). "A case of infantile osteopetrosis: The radioclinical features with literature update". Bone Rep. 4: 11–16. doi:10.1016/j.bonr.2015.11.002. PMC 4926827. PMID 28326337.
{{cite journal}}: CS1 maint: multiple names: authors list (link) - ↑ Orchard PJ, Fasth AL, Le Rademacher J, He W, Boelens JJ, Horwitz EM; et al. (2015). "Hematopoietic stem cell transplantation for infantile osteopetrosis". Blood. 126 (2): 270–6. doi:10.1182/blood-2015-01-625541. PMC 4497967. PMID 26012570.
{{cite journal}}: CS1 maint: multiple names: authors list (link) - ↑ Elsobky TA, El-Haddad A, Elsobky E, Elsayed SM, Sakr HM (2017). "Reversal of skeletal radiographic pathology in a case of malignant infantile osteopetrosis following hematopoietic stem cell transplantation". Egypt J Radiol Nucl Med. 48 (1): 237–43. doi:10.1016/j.ejrnm.2016.12.013.
{{cite journal}}: CS1 maint: multiple names: authors list (link) - ↑ Hashemi Taheri AP, Radmard AR, Kooraki S, Behfar M, Pak N, Hamidieh AA; et al. (2015). "Radiologic resolution of malignant infantile osteopetrosis skeletal changes following hematopoietic stem cell transplantation". Pediatr Blood Cancer. 62 (9): 1645–9. doi:10.1002/pbc.25524. PMID 25820806. S2CID 11287381.
{{cite journal}}: CS1 maint: multiple names: authors list (link) - ↑ "Archive copy". Archived from the original on 2021-11-05. Retrieved 2021-12-27.
{{cite web}}: CS1 maint: archived copy as title (link) - ↑ Allen, Matthew R.; Burr, David B. (2014). Basic and Applied Bone Biology. San diego: Academic Press. pp. 75–90. ISBN 9780124160156.
- ↑ Memet, Aker; Rouvinski, Alex; Hshavia, Saar; Ta-Shma, Asaf; Shaag, Avraham; Zenvirt, Shamir; Israel, Shoshana; Weintraub, Michael; Taraboulos, Albert; Bar-Shavit, Zvi; Elpeleg, Orly (April 2012). "An SNX10 mutation causes malignant osteoporosis of infancy". Journal of Medical Genetics. 49 (4): 221–6. doi:10.1136/jmedgenet-2011-100520. PMID 22499339. Archived from the original on December 13, 2017. Retrieved August 19, 2016.
- ↑ Askmyr MK et al.: Towards a better understanding and new therapeutics of osteopetrosis. Br J Haematol 140:597, 208
- ↑ Robbins Basic Pathology by Kumar, Abbas, Fausto, and Mitchell, 8th edition
- 1 2 3 Reference, Genetics Home. "osteopetrosis". Genetics Home Reference. Archived from the original on 2017-12-22. Retrieved 2017-12-13.
- ↑ Ihde LL, Forrester DM, Gottsegen CJ, Masih S, Patel DB, Vachon LA; et al. (2011). "Sclerosing bone dysplasias: Review and differentiation from other causes of osteosclerosis". RadioGraphics. 31 (7): 1865–82. doi:10.1148/rg.317115093. PMID 22084176.
{{cite journal}}: CS1 maint: multiple names: authors list (link) - ↑ "Osteopetrosis | Genetic and Rare Diseases Information Center (GARD) – an NCATS Program". rarediseases.info.nih.gov. Archived from the original on 2017-12-13. Retrieved 2017-12-13.
- 1 2 "Osteopetrosis - NORD (National Organization for Rare Disorders)". NORD (National Organization for Rare Disorders). Archived from the original on 2018-02-07. Retrieved 2017-12-13.
- ↑ "ghr.nlm.nih.gov/condition/osteopetrosis". Archived from the original on 2020-09-21. Retrieved 2021-12-27.
- ↑ "Центр Молекулярной Генетики". Archived from the original on 2021-05-14. Retrieved 2021-12-27.
- ↑ Медицинская генетика Чувашии Archived February 1, 2016, at the Wayback Machine
- ↑ Lo Iacono, Nadia; Blair, Harry C.; Poliani, Pietro L.; Marrella, Veronica; Ficara, Francesca; Cassani, Barbara; Facchetti, Fabio; Fontana, Elena; Guerrini, Matteo M. (December 2012). "Osteopetrosis rescue upon RANKL administration to Rankl(-/-) mice: a new therapy for human RANKL-dependent ARO". Journal of Bone and Mineral Research. 27 (12): 2501–2510. doi:10.1002/jbmr.1712. ISSN 1523-4681. PMID 22836362.
- ↑ "Archive copy". Archived from the original on 2021-11-23. Retrieved 2021-12-27.
{{cite web}}: CS1 maint: archived copy as title (link) - ↑ Maddan, Heather (2007-09-23). "Marin County artist Laurel Burch dead at 61 of rare bone disease". The San Francisco Chronicle. Archived from the original on 2007-10-05. Retrieved 2007-12-23.
Bibliography
- Penna, Sara; Capo, Valentina; Palagano, Eleonora; Sobacchi, Cristina; Villa, Anna (19 February 2019). "One Disease, Many Genes: Implications for the Treatment of Osteopetroses". Frontiers in Endocrinology. 10: 85. doi:10.3389/fendo.2019.00085. PMC 6389615. PMID 30837952.
- Susani, Lucia; Pangrazio, Alessandra; Sobacchi, Cristina; Taranta, Anna; Mortier, Geert; Savarirayan, Ravi; Villa, Anna; Orchard, Paul; Vezzoni, Paolo; Albertini, Alberto; Frattini, Annalisa; Pagani, Franco (September 2004). "TCIRG1-dependent recessive osteopetrosis: Mutation analysis, functional identification of the splicing defects, andin vitro rescue by U1 snRNA". Human Mutation. 24 (3): 225–235. doi:10.1002/humu.20076. PMID 15300850. S2CID 31788054.
- GeneReviews/NCBI/NIH/UW entry on CLCN7-Related Osteopetrosis Archived 2010-06-02 at the Wayback Machine
External links
| Classification | |
|---|---|
| External resources |