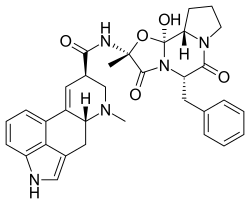
Ergotamine
Ergotamine, sold under the brand names Cafergot (with caffeine) and Ergomar among others, is an ergopeptine and part of the ergot family of alkaloids; it is structurally and biochemically closely related to ergoline.[5] It possesses structural similarity to several neurotransmitters, and has biological activity as a vasoconstrictor.
 | |
 | |
| Clinical data | |
|---|---|
| Trade names | Cafergot (with caffeine), Ergomar, others |
| Other names | 2'-Methyl-5'α-benzyl-12'-hydroxy-3',6',18-trioxoergotaman; 9,10α-Dihydro-12'-hydroxy-2'-methyl-5'α-(phenylmethyl)ergotaman-3',6',18-trione |
| AHFS/Drugs.com | Monograph |
| Routes of administration | Oral |
| ATC code | |
| Legal status | |
| Legal status |
|
| Pharmacokinetic data | |
| Bioavailability | Intravenous: 100%,[2] Intramuscular: 47%,[3] Oral: <1%[4] (Enhanced by co-administration of caffeine[2]) |
| Metabolism | Hepatic[3] |
| Elimination half-life | 2 hours[3] |
| Excretion | 90% biliary[3] |
| Identifiers | |
| |
| CAS Number | |
| PubChem CID | |
| IUPHAR/BPS | |
| DrugBank | |
| ChemSpider | |
| UNII | |
| KEGG | |
| ChEBI | |
| ChEMBL | |
| PDB ligand | |
| CompTox Dashboard (EPA) | |
| ECHA InfoCard | 100.003.658 |
| Chemical and physical data | |
| Formula | C33H35N5O5 |
| Molar mass | 581.673 g·mol−1 |
| 3D model (JSmol) | |
| |
| |
| | |
It is used medicinally for treatment of acute migraine attacks (sometimes in combination with caffeine). Medicinal usage of ergot fungus began in the 16th century to induce childbirth, yet dosage uncertainties discouraged the use. It has been used to prevent post-partum hemorrhage (bleeding after childbirth). It was first isolated from the ergot fungus by Arthur Stoll at Sandoz in 1918 and marketed as Gynergen in 1921.[6]
Biosynthesis
Ergotamine is a secondary metabolite (natural product) and the principal alkaloid produced by the ergot fungus, Claviceps purpurea, and related fungi in the family Clavicipitaceae.[7] Its biosynthesis in these fungi requires the amino acid L-tryptophan and dimethylallyl pyrophosphate. These precursor compounds are the substrates for the enzyme, tryptophan dimethylallyltransferase, catalyzing the first step in ergot alkaloid biosynthesis, i.e., the prenylation of L-tryptophan. Further reactions, involving methyltransferase and oxygenase enzymes, yield the ergoline, lysergic acid. Lysergic acid (LA) is the substrate of lysergyl peptide synthetase, a nonribosomal peptide synthetase, which covalently links LA to the amino acids, L-alanine, L-proline, and L-phenylalanine. Enzyme-catalyzed or spontaneous cyclizations, oxygenations/oxidations, and isomerizations at selected residues precede, and give rise to, formation of ergotamine.[8]
Medical uses
Ergotamine continues to be prescribed for migraines and cluster headaches.[9]
Availability and dosage
In the United States, ergotamine is available as a suppository, a sublingual tablet, and a tablet, sometimes in combination with caffeine. The suppository is available under the brand name Migergot, which contains 2 mg of ergotamine with 100 mg caffeine. The sublingual tablet is available under the brand name Ergomar and contains 2 mg of ergotamine. The combination tablet in combination with caffeine called Cafergot contains 1 mg of ergotamine and 100 mg of caffeine.[10]
This preparation may be used immediately following the aura/onset of pain to abort the migraine. For the best results, dosage should start at the first sign of an attack.[11]
Contraindications
Contraindications include: atherosclerosis, Buerger's syndrome, coronary artery disease, hepatic disease, pregnancy, pruritus, Raynaud's syndrome, and renal disease.[12] It's also contraindicated if patient is taking macrolide antibiotics (e.g., erythromycin), certain HIV protease inhibitors (e.g., ritonavir, nelfinavir, indinavir), certain azole antifungals (e.g., ketoconazole, itraconazole, voriconazole) delavirdine, efavirenz, or a 5-HT1 receptor agonist (e.g., sumatriptan). [13]
Side effects
Side effects of ergotamine include nausea and vomiting. At higher doses, it can cause raised arterial blood pressure, vasoconstriction (including coronary vasospasm) and bradycardia or tachycardia. Severe vasoconstriction may cause symptoms of intermittent claudication.[14][9]
Pharmacology
Pharmacodynamics
Ergotamine interacts with serotonin, adrenergic, and dopamine receptors.[15][16] It is an agonist of serotonin receptors including the 5-HT1 and 5-HT2 subtypes.[15] Ergotamine is an agonist of the serotonin 5-HT2B receptor and has been associated with cardiac valvulopathy.[17] Despite acting as a potent 5-HT2A receptor agonist, ergotamine is said to be non-hallucinogenic similarly to lisuride.[18][19] This is thought to be due to functional selectivity at the 5-HT2A receptor.[18][19]
| Site | Affinity (Ki/IC50 [nM]) | Efficacy (Emax [%]) | Action |
|---|---|---|---|
| 5-HT1A | 0.17–0.3 | ? | Full agonist |
| 5-HT1B | 0.3–4.7 | ? | Agonist |
| 5-HT1D | 0.3–6.0 | ? | Agonist |
| 5-HT1E | 19–840 | ? | ? |
| 5-HT1F | 170–171 | ? | ? |
| 5-HT2A | 0.64–0.97 | ? | Full agonist |
| 5-HT2B | 1.3–45 | ? | Partial agonist |
| 5-HT2C | 1.9–9.8 | ? | Partial agonist |
| 5-HT3 | >10,000 | – | – |
| 5-HT4 | 65 | ? | ? |
| 5-HT5A | 14 | ? | Agonist |
| 5-HT5B | 3.2–16 | ? | ? |
| 5-HT6 | 12 | ? | ? |
| 5-HT7 | 1,291 | ? | Agonist |
| α1A | 15–>10,000 | – | – |
| α1B | 12–>10,000 | – | – |
| α1D | ? | ? | ? |
| α2A | 106 | ? | ? |
| α2B | 88 | ? | ? |
| α2C | >10,000 | – | – |
| β1 | >10,000 | – | – |
| β2 | >10,000 | – | – |
| D1 | >10,000 | – | – |
| D2 | 4.0–>10,000 | – | Agonist |
| D3 | 3.2–>10,000 | – | – |
| D4 | 12–>10,000 | – | – |
| D5 | 170 | ? | ? |
| H1 | >10,000 | – | – |
| H2 | >10,000 | – | – |
| M1 | 862 | ? | ? |
| M2 | 911 | ? | ? |
| M3 | >10,000 | – | – |
| M4 | >10,000 | – | – |
| M5 | >10,000 | – | – |
| Notes: All receptors are human except 5-HT5A (mouse/rat) and 5-HT5B (mouse/rat—no human counterpart).[16] No affinity for histamine H1 or H2, cannabinoid CB1, GABA, glutamate, or nicotinic acetylcholine receptors, nor the monoamine transporters (all >10,000 nM).[16] | |||
Pharmacokinetics
The bioavailability of ergotamine is around 2% orally, 6% rectally, and 100% by intramuscular or intravenous injection.[15] The low oral and rectal bioavailability is due to low gastrointestinal absorption and high first-pass metabolism.[15]
Legal status
Ergotamine is included as a List I precursor in the United States, as it is a commonly used precursor for the production of LSD.[24]
See also
References
- Anvisa (2023-03-31). "RDC Nº 784 - Listas de Substâncias Entorpecentes, Psicotrópicas, Precursoras e Outras sob Controle Especial" [Collegiate Board Resolution No. 784 - Lists of Narcotic, Psychotropic, Precursor, and Other Substances under Special Control] (in Brazilian Portuguese). Diário Oficial da União (published 2023-04-04). Archived from the original on 2023-08-03. Retrieved 2023-08-15.
- Sanders SW, Haering N, Mosberg H, Jaeger H (1986). "Pharmacokinetics of ergotamine in healthy volunteers following oral and rectal dosing". European Journal of Clinical Pharmacology. 30 (3): 331–334. doi:10.1007/BF00541538. PMID 3732370. S2CID 37538721.
- Tfelt-Hansen P, Johnson ES (1993). "Ergotamine". In Olesen J, Tfelt-Hansen P, Welch KM (eds.). The Headaches. New York: Raven Press. pp. 313–22.
- Ibraheem JJ, Paalzow L, Tfelt-Hansen P (December 1983). "Low bioavailability of ergotamine tartrate after oral and rectal administration in migraine sufferers". British Journal of Clinical Pharmacology. 16 (6): 695–699. doi:10.1111/j.1365-2125.1983.tb02243.x. PMC 1428366. PMID 6419759.
- Index Nominum 2000: International Drug Directory. Taylor & Francis. 2000. pp. 397–. ISBN 978-3-88763-075-1.
- AJ Giannini, AE Slaby. Drugs of Abuse. Oradell, NJ, Medical Economics Books, 1989.
- "Pharmacognosy of Ergot (Argot or St. Anthony's Fire)". pharmaxchange.info. 30 December 2011. Archived from the original on 17 July 2012.
- Schardl CL, Panaccione DG, Tudzynski P (2006). "Ergot alkaloids--biology and molecular biology". The Alkaloids. Chemistry and Biology. 63: 45–86. doi:10.1016/S1099-4831(06)63002-2. ISBN 978-0-12-469563-4. PMID 17133714.
- Zajdel P, Bednarski M, Sapa J, Nowak G (April 2015). "Ergotamine and nicergoline - facts and myths". Pharmacological Reports. 67 (2): 360–363. doi:10.1016/j.pharep.2014.10.010. PMID 25712664. S2CID 22768662.
- "Approved Drug Products". FDA Orange Book (40th ed.). U.S. Food and Drug Administration. 2020.
- "CAFERGOT- ergotamine tartrate and caffeine tablet, film coated". DailyMed. U.S. National Library of Medicine. Archived from the original on 2014-01-16.
- Giannini AJ (1986). Biological Foundations of Clinical Psychiatry. Oradell, NJ: Medical Economics Publishing Co.
- "Ergotamine: Indications, Side Effects, Warnings". Drugs.com. Archived from the original on 25 March 2017. Retrieved 25 March 2017.
- "Medihaler Ergotamine". drugs.com. Archived from the original on 2016-04-01. Retrieved 2016-05-20.
- Ramírez Rosas MB, Labruijere S, Villalón CM, Maassen Vandenbrink A (August 2013). "Activation of 5-hydroxytryptamine1B/1D/1F receptors as a mechanism of action of antimigraine drugs". Expert Opinion on Pharmacotherapy. 14 (12): 1599–1610. doi:10.1517/14656566.2013.806487. PMID 23815106. S2CID 22721405.
- PDSP Database – UNC
- Cavero I, Guillon JM (2014). "Safety Pharmacology assessment of drugs with biased 5-HT(2B) receptor agonism mediating cardiac valvulopathy". Journal of Pharmacological and Toxicological Methods. 69 (2): 150–161. doi:10.1016/j.vascn.2013.12.004. PMID 24361689.
- Karaki S, Becamel C, Murat S, Mannoury la Cour C, Millan MJ, Prézeau L, et al. (May 2014). "Quantitative phosphoproteomics unravels biased phosphorylation of serotonin 2A receptor at Ser280 by hallucinogenic versus nonhallucinogenic agonists". Molecular & Cellular Proteomics. 13 (5): 1273–1285. doi:10.1074/mcp.M113.036558. PMC 4014284. PMID 24637012.
- Hanks J, González-Maeso J (2016). "Molecular and Cellular Basis of Hallucinogen Action". In Preedy VR (ed.). Neuropathology of Drug Addictions and Substance Misuse. Vol. 2: Stimulants, Club and Dissociative Drugs, Hallucinogens, Steroids, Inhalants and International Aspects. pp. 803–812. doi:10.1016/B978-0-12-800212-4.00075-3. ISBN 978-0-12-800212-4.
- Silberstein SD, McCrory DC (February 2003). "Ergotamine and dihydroergotamine: history, pharmacology, and efficacy". Headache. 43 (2): 144–166. doi:10.1046/j.1526-4610.2003.03034.x. PMID 12558771. S2CID 21356727.
- Rothman RB, Baumann MH, Savage JE, Rauser L, McBride A, Hufeisen SJ, Roth BL (December 2000). "Evidence for possible involvement of 5-HT(2B) receptors in the cardiac valvulopathy associated with fenfluramine and other serotonergic medications". Circulation. 102 (23): 2836–2841. doi:10.1161/01.cir.102.23.2836. PMID 11104741.
- Rubio-Beltrán E, Labastida-Ramírez A, Haanes KA, van den Bogaerdt A, Bogers AJ, Zanelli E, et al. (December 2019). "Characterization of binding, functional activity, and contractile responses of the selective 5-HT1F receptor agonist lasmiditan". British Journal of Pharmacology. 176 (24): 4681–4695. doi:10.1111/bph.14832. PMC 6965684. PMID 31418454.
- Pytliak M, Vargová V, Mechírová V, Felšöci M (2011). "Serotonin receptors - from molecular biology to clinical applications". Physiological Research. 60 (1): 15–25. doi:10.33549/physiolres.931903. PMID 20945968.
- "Lists of: Scheduling Actions, Controlled Substances, Regulated Chemicals" (PDF). Drug Enforcement Administration, Diversion Control Division, Drug & Chemical Evaluation Section. U.S. Department of Justice. February 2020.