Repinotan
 | |
| Clinical data | |
|---|---|
| Routes of administration | Oral |
| Legal status | |
| Legal status |
|
| Identifiers | |
IUPAC name
| |
| CAS Number | |
| PubChem CID | |
| IUPHAR/BPS | |
| ChemSpider | |
| UNII | |
| ChEMBL | |
| CompTox Dashboard (EPA) | |
| Chemical and physical data | |
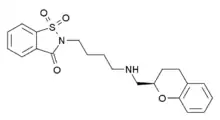
| Formula | C21H24N2O4S |
| Molar mass | 400.49 g·mol−1 |
| 3D model (JSmol) | |
SMILES
| |
InChI
| |
| | |
Repinotan (BAYx3702), an aminomethylchroman derivative, is a selective 5-HT1A receptor full agonist with high potency and efficacy.[1][2] It has neuroprotective effects in animal studies,[3][4][5] and was trialed in humans for reducing brain injury following head trauma.[6] It was subsequently trialed up to phase II for treatment of stroke, but while side effects were mild and consisted mainly of nausea, repinotan failed to demonstrate sufficient efficacy to justify further clinical trials.[7][8][9] However, repinotan continues to be investigated for other applications, and was found to be effective at counteracting the respiratory depression produced by morphine, though with slight reduction in analgesic effects.[10]
History
Bayer Healthcare AG (Wuppertal, Germany) first synthesized repinotan during early 2000s. As of 2004, it was expected to be filed by the NDA. Phase III trials for both ischemic stroke and traumatic brain injury were run in March 2002.[11] However, these trials found the drug ineffective as a treatment (November, 2009).[12]
In October 2010, further investigation showed repinotan able to counteract respiratory depression caused by morphine. Repinotan continues to be examined, but has not yet been commercially released.[10]
Chemical and Physical Properties
Repinotan is an enantiomerically pure aminomethyl chromane derivative with a saccharinylbutyl substituent.[13] It is classified as a synthetic organic and possesses five hydrogen bond acceptors and one hydrogen bond donor. Its topological polar surface area is 84.09 and it has seven rotatable bonds. In addition, its molecular weight is 400.15 g/mole. Repinotan has a formal charge of zero and a covalently-bonded unit count of one. It is similar in chemical and physical properties to the ligands quetiapine, PAT5A, and pioglitazone.[14]
Synthesis
Bayer Healthcare AG synthesized Repinotan in three main reaction sequences. A form with a metabolically stable 14carbon-label was necessary for pharmacokinetic studies. The hydrochloride was hydroxylated in the 6-position of the chromane moiety.[13]
First Reaction Scheme
For the first reaction sequence, [14C]-phenol was used as the starting compound. Michael adduct formation was then employed in the preparation of chromane rings with [14C]-phenol.[13]
Second Reaction Scheme
In the second reaction sequence, [Carbonyl-14C]-2-hydroxy-acetophenone was used first. Compound XII was formed from condensation of [carbonyl-14C-]-2-hydroxy-acetophenone with dimethyl oxylate and ring closure. Hydrogenolytical debenzylation and hydrochloric acid created the final product.[13]
Third Reaction Scheme
The third reaction involved intermediate XVII undergoing acylation using acetyl chloride. Deacetylation and debenzylation were then implemented with HCI. Pd/C was used in the deacetylation step and Pd/C was used in the debenzylation step.[13]
Mechanism of Action
Repinotan HCI (BAYx3702) acts as a highly selective 5-HT1A receptor full agonist. It is blocked by the specific 5-HT1A receptor antagonist, WAY 100135 [10] and its primary metabolizer is CYP2D6. Ethnic differences are known to have an effect on CYP2D6. Repinotan is believed to operate through neuronal hyperpolarization.[15]
When repinotan first binds to both pre- and post-synaptic 5-HT1A receptors, G protein-coupled inwardly rectifying K+ channels are activated. This causes hyperpolarization. Because hyperpolarization causes inhibition of neuron firing and less glutamate release, neurons are protected against overexcitation. This could explain repinotan's neuroprotective properties.[8]
In addition, the protein Bcl-2, the serotonergic glial growth factor S-100beta, and Nerve Growth Factor are affected by repinotan.[8] Repinotan is able to suppress caspase-3 through MAPK and PKCalpha.[16] Apoptosis as a result of anoxia/reoxygenation and H(2)O(2) treatment may also be inhibited.[17]
Repinotan has been found to bind with high to moderate affinity to the receptors alpha-1 and alpha-2 adrenergic, 5-HT7- and 5-HT1D, dopamine D2 and D4, sigma sites, and 5-HT2C. It is able to increase activity of VTA dopaminergic neurons and medial prefrontal cortex dopamine release.[18]
Pharmacology
Pharmacodynamics
Repinotan acts as a selective high-affinity full receptor agonist at the 5-HT1A receptor subtype.[12] It increases the activity of dopamine (DA) neurons in the ventral tegmental area as well as DA release in the medial prefrontal cortex.[19]
Additionally, it is an extremely potent drug and is able to cross the blood-brain barrier. After infusion, the distribution equilibrium between plasma and brain is reached almost instantaneously.[20]
Repinotan's efficacy is mainly dependent on factors such as the length of time between the start of stroke symptoms and taking the drug. The age and blood pressure of the patient also plays a role. Decreases in response with increasing age as well as decreases in response as blood pressure increases are generally observed.[21] The most efficient dose is approximately 1.25 mg per day.[22]
Pharmacokinetics
Repinotan's primary route of administration is by intravenous injection,[12] which indicates that it goes directly into the bloodstream. It is able to cross the blood-brain barrier- a highly selective barrier that separates circulating blood from the brain's extracellular fluid. Diffusion acts as the driving force, which allows repinotan to cross in both directions. In addition, the drug is uncharged, which is consistent with the fact that it is able to pass the lipophilic and non-polar blood-brain barrier.[20]
The half-life of repinotan is approximately 1 hour. Elimination ensues in parallel from plasma and brain. In addition, repinotan's volume of distribution at steady-state and plasma clearance are independent of dose. This is indicative of linear pharmacokinetics over the range of 0.1-3.0 micrograms repinotan/kg/h.[23]
Infusion rates of up to 150 microg/h are well received.[24] Repinotan's optimal dose is 1.25 mg/day.[22]
Potential Effects of Gender and Age on Repinotan's Administration
Gender and age do not have any influence on repinotan's pharmacokinetics. Bodyweight also does not play a big role.[24]
Treatment
Acute Ischemic Stroke
Repinotan was originally developed by Bayer Healthcare AG (Wuppertal, Germany) as an oral treatment for depression.[11] However, it was instead trialed as a candidate for reducing brain injury following head trauma. The drug was then examined as a preventative of secondary brain damage for ischemic stroke victims. Early trials showed repinotan's ability to reduce hippocampal CA1 and CA3 neuronal loss. Cortical tissue damage was also reduced. In addition, repinotan was shown to mitigate spatial learning deficits.[25] However, trials were discontinued due to repinotan's efficacy being insufficient.[12]
Respiratory Depression

Repinotan has presently been found to be effective at stopping respiratory depression caused by morphine. In addition, it represses nociception at high doses, but enhances nociception at small doses (0.2 micrograms/kg).[10] Repinotan may be applicable to Parkinson's, as it is able to reduce glutamate-induced excitotoxicity and thereby some cell death.[26]
Additional Medications Trialed
Another stroke medication trialed at the same time, picozotan, is similar to repinotan in that it is also a serotonin agonist. Other drugs included zonampanel, which acts as an AMPA receptor antagonist instead of a 5-HT1A receptor agonist and DP-b99. DP-b99 is a metal iron chelator.[27]
Side Effects
Repinotan's side effects during trials as a treatment for ischemic stroke consisted mainly of serotonergic side effects including nausea and vomiting. The most common side effect was headache. Neurological worsening, cerebral hemorrhage, and brain edema were the most common severe effects. However, repinotan was generally shown to be safe.[22]
Its current investigation as an antagonist for respiratory depression caused by morphine has shown there to be no serious cardiovascular side effects. However, a slight decrease in blood pressure was a more minor effect.[10] Repinotan has been linked with pupil diameter reduction.[28]
Original Predictions and Current Availability
Currently, repinotan is not commercially available in the United States. Sales of $1000 million in the U.S. and a launch date of 2006 were originally anticipated by Lehman Brothers. Bank Vontobel and Bayer both estimated sales of 450 million Euros. However, the drug continues to be under investigation for different treatments than its original intent.[11]
See also
References
- ↑ De Vry, J.; Schohe-Loop, R.; Heine, H. G.; Greuel, J. M.; Mauler, F.; Schmidt, B.; Sommermeyer, H.; Glaser, T. (1998). "Characterization of the aminomethylchroman derivative BAY x 3702 as a highly potent 5-hydroxytryptamine1A receptor agonist". The Journal of Pharmacology and Experimental Therapeutics. 284 (3): 1082–1094. PMID 9495870.
- ↑ Dong, J.; De Montigny, C.; Blier, P. (1998). "Full agonistic properties of BAY x 3702 on presynaptic and postsynaptic 5-HT1A receptors electrophysiological studies in the rat hippocampus and dorsal raphe". The Journal of Pharmacology and Experimental Therapeutics. 286 (3): 1239–1247. PMID 9732384.
- ↑ Alessandri, B.; Tsuchida, E.; Bullock, R. M. (1999). "The neuroprotective effect of a new serotonin receptor agonist, BAY X3702, upon focal ischemic brain damage caused by acute subdural hematoma in the rat". Brain Research. 845 (2): 232–235. doi:10.1016/S0006-8993(99)01948-4. PMID 10536203. S2CID 36341439.
- ↑ Kline, A. E.; Yu, J.; Horváth, E.; Marion, D. W.; Dixon, C. E. (2001). "The selective 5-HT(1A) receptor agonist repinotan HCl attenuates histopathology and spatial learning deficits following traumatic brain injury in rats". Neuroscience. 106 (3): 547–555. doi:10.1016/S0306-4522(01)00300-1. PMID 11591455. S2CID 54308982.
- ↑ Mauler, F.; Horváth, E. (2005). "Neuroprotective efficacy of repinotan HCl, a 5-HT1A receptor agonist, in animal models of stroke and traumatic brain injury". Journal of Cerebral Blood Flow and Metabolism. 25 (4): 451–459. doi:10.1038/sj.jcbfm.9600038. PMID 15674237.
- ↑ Ohman, J.; Braakman, R.; Legout, V.; Traumatic Brain Injury Study Group (2001). "Repinotan (BAY x 3702): a 5HT1A agonist in traumatically brain injured patients". Journal of Neurotrauma. 18 (12): 1313–1321. doi:10.1089/08977150152725614. PMID 11780862.
- ↑ Lutsep, H. L. (2005). "Repinotan, A 5-HT1A agonist, in the treatment of acute ischemic stroke". Current Drug Targets. CNS and Neurological Disorders. 4 (2): 119–120. doi:10.2174/1568007053544165. PMID 15857296.
- 1 2 3 Berends AC, Luiten PG, Nyakas C (2005). "A review of the neuroprotective properties of the 5-HT1A receptor agonist repinotan HCl (BAYx3702) in ischemic stroke". CNS Drug Rev. 11 (4): 379–402. doi:10.1111/j.1527-3458.2005.tb00055.x. PMC 6741728. PMID 16614737.
- ↑ Teal, P.; Davis, S.; Hacke, W.; Kaste, M.; Lyden, P.; Modified Randomized Exposure Controlled Trial Study Investigators; Fierus, M.; Bayer Healthcare, A. (2009). "A randomized, double-blind, placebo-controlled trial to evaluate the efficacy, safety, tolerability, and pharmacokinetic/pharmacodynamic effects of a targeted exposure of intravenous repinotan in patients with acute ischemic stroke: modified Randomized Exposure Controlled Trial (mRECT)". Stroke: A Journal of Cerebral Circulation. 40 (11): 3518–3525. doi:10.1161/STROKEAHA.109.551382. PMID 19745176.
- 1 2 3 4 5 Guenther U, Wrigge H, Theuerkauf N, Boettcher MF, Wensing G, Zinserling J, Putensen C, Hoeft A (October 2010). "Repinotan, a selective 5-HT1A-R-agonist, antagonizes morphine-induced ventilatory depression in anesthetized rats". Anesth. Analg. 111 (4): 901–7. doi:10.1213/ANE.0b013e3181eac011. PMID 20802053. S2CID 39217801.
- 1 2 3 Lutsep, HL (June 2002). "Repinotan Bayer". Current Opinion in Investigational Drugs. 3 (6): 924–7. PMID 12137415.
- 1 2 3 4 Teal, P; Davis, S; Hacke, W; Kaste, M; Lyden, PD; Modified Randomized Exposure Controlled Trial Study, Investigators; Fierus, M; Bayer HealthCare, AG (November 2009). "A randomized, double-blind, placebo-controlled trial to evaluate the efficacy, safety, tolerability, and pharmacokinetic/pharmacodynamic effects of a targeted exposure of intravenous repinotan in patients with acute ischemic stroke: modified Randomized Exposure Controlled Trial (mRECT)". Stroke: A Journal of Cerebral Circulation. 40 (11): 3518–25. doi:10.1161/strokeaha.109.551382. PMID 19745176.
- 1 2 3 4 5 Seidel, D.; Conrad, M.; Schoof, Y.; Schohe-Loop, R. (November 2002). "Synthesis of [14C]-labelled repinotan hydrochloride and its major metabolite M-6". Journal of Labelled Compounds and Radiopharmaceuticals. 45 (13): 1115–1132. doi:10.1002/jlcr.629.
- ↑ "PubChem- Repinotan". Pubchem. National Center for Biotechnology Information, U.S. National Library of Medicine. Retrieved 10 November 2014.
- ↑ Tanigawa, T; Heinig, R; Kuroki, Y; Higuchi, S (February 2006). "Evaluation of interethnic differences in repinotan pharmacokinetics by using population approach" (PDF). Drug Metabolism and Pharmacokinetics. 21 (1): 61–69. doi:10.2133/dmpk.21.61. PMID 16547395. S2CID 10517194. Archived from the original (PDF) on 2020-02-07.
- ↑ De Vry, J; Schohe-Loop, R; Heine, HG; Greuel, JM; Mauler, F; Schmidt, B; Sommermeyer, H; Glaser, T (March 1998). "Characterization of the aminomethylchroman derivative BAY x 3702 as a highly potent 5-hydroxytryptamine1A receptor agonist". The Journal of Pharmacology and Experimental Therapeutics. 284 (3): 1082–94. PMID 9495870.
- ↑ Adayev, T; Ray, I; Sondhi, R; Sobocki, T; Banerjee, P (7 April 2003). "The G protein-coupled 5-HT1A receptor causes suppression of caspase-3 through MAPK and protein kinase Calpha". Biochimica et Biophysica Acta (BBA) - Molecular Cell Research. 1640 (1): 85–96. doi:10.1016/s0167-4889(03)00023-5. PMID 12676358.
- ↑ Díaz-Mataix, L; Artigas, F; Celada, P (May 2006). "Activation of pyramidal cells in rat medial prefrontal cortex projecting to ventral tegmental area by a 5-HT1A receptor agonist". European Neuropsychopharmacology. 16 (4): 288–96. doi:10.1016/j.euroneuro.2005.10.003. hdl:10261/34586. PMID 16290106. S2CID 38788669.
- ↑ Díaz-Mataix, L; Scorza, MC; Bortolozzi, A; Toth, M; Celada, P; Artigas, F (23 November 2005). "Involvement of 5-HT1A receptors in prefrontal cortex in the modulation of dopaminergic activity: role in atypical antipsychotic action" (PDF). The Journal of Neuroscience. 25 (47): 10831–43. doi:10.1523/jneurosci.2999-05.2005. PMC 6725886. PMID 16306396.
- 1 2 Schwarz, T; Beckermann, B; Buehner, K; Mauler, F; Schuhmacher, J; Seidel, D; Steinke, W; Weinz, C; Zimmerd, D (September 2005). "Pharmacokinetics of repinotan in healthy and brain injured animals". Biopharmaceutics & Drug Disposition. 26 (6): 259–68. doi:10.1002/bdd.458. PMID 15966026. S2CID 25596274.
- ↑ Teal, P.; Davis, S.; Hacke, W.; Kaste, M.; Lyden, P. D.; Fierus, M. (10 September 2009). "A Randomized, Double-Blind, Placebo-Controlled Trial to Evaluate the Efficacy, Safety, Tolerability, and Pharmacokinetic/Pharmacodynamic Effects of a Targeted Exposure of Intravenous Repinotan in Patients With Acute Ischemic Stroke: Modified Randomized Exposure Controlled Trial (mRECT)". Stroke. 40 (11): 3518–3525. doi:10.1161/STROKEAHA.109.551382. PMID 19745176.
- 1 2 3 Teal, P; Silver, FL; Simard, D (February 2005). "The BRAINS study: safety, tolerability, and dose-finding of repinotan in acute stroke". The Canadian Journal of Neurological Sciences. 32 (1): 61–7. doi:10.1017/s0317167100016899. PMID 15825548.
- ↑ Heinig, R; Sundaresan, P; Shah, A; Boettcher, M (2005). "Effect of gender and age on the pharmacokinetics of repinotan". Clinical Drug Investigation. 25 (2): 125–34. doi:10.2165/00044011-200525020-00005. PMID 17523762. S2CID 40485277.
- 1 2 Heinig, R; Böttcher, MF (2005). "Pharmacokinetics of escalating doses of intravenous repinotan in healthy male volunteers". Clinical Drug Investigation. 25 (2): 115–23. doi:10.2165/00044011-200525020-00004. PMID 17523761. S2CID 23415230.
- ↑ Kline, AE; Yu, J; Horváth, E; Marion, DW; Dixon, CE (2001). "The selective 5-HT(1A) receptor agonist repinotan HCl attenuates histopathology and spatial learning deficits following traumatic brain injury in rats". Neuroscience. 106 (3): 547–55. doi:10.1016/s0306-4522(01)00300-1. PMID 11591455. S2CID 54308982.
- ↑ Bezard, E; Gerlach, I; Moratalla, R; Gross, CE; Jork, R (July 2006). "5-HT1A receptor agonist-mediated protection from MPTP toxicity in mouse and macaque models of Parkinson's disease". Neurobiology of Disease. 23 (1): 77–86. doi:10.1016/j.nbd.2006.02.003. hdl:10261/59551. PMID 16545572. S2CID 19803633.
- ↑ Ferro, JM; Dávalos, A (2006). "Other neuroprotective therapies on trial in acute stroke". Cerebrovascular Diseases. 21 Suppl 2 (2): 127–30. doi:10.1159/000091712. PMID 16651823. S2CID 39193793.
- ↑ Boettcher, M; Heinig, R; Wensing, G; Kuhlmann, J (March 2005). "Pupil reaction: a valid sensitive clinical biomarker for 5-HT compounds". Basic & Clinical Pharmacology & Toxicology. 96 (3): 246. doi:10.1111/j.1742-7843.2005.pto960317.x. PMID 15733223.