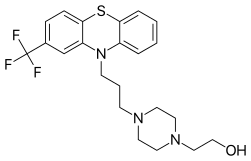
Fluphenazine
 | |
 | |
| Names | |
|---|---|
| Trade names | Prolixin, Modecate, Moditen others |
IUPAC name
| |
| Clinical data | |
| WHO AWaRe | UnlinkedWikibase error: ⧼unlinkedwikibase-error-statements-entity-not-set⧽ |
| Pregnancy category |
|
| Routes of use | by mouth, IM, depot injection (fluphenazine decanoate) |
| Defined daily dose | 10 mg (by mouth) 1 mg (injection)[1] |
| External links | |
| AHFS/Drugs.com | Monograph |
| MedlinePlus | a682172 |
| Legal | |
| License data |
|
| Legal status | |
| Pharmacokinetics | |
| Bioavailability | 2.7% (by mouth) |
| Metabolism | unclear[2] |
| Elimination half-life | IM 15 hours (HCL), 7-10 days (decanoate)[2] |
| Excretion | Urine, faeces |
| Chemical and physical data | |
| Formula | C22H26F3N3OS |
| Molar mass | 437.53 g·mol−1 |
| 3D model (JSmol) | |
SMILES
| |
InChI
| |
Fluphenazine, sold under the brand names Prolixin among others, is an antipsychotic medication.[2] It is used in the treatment of chronic psychoses such as schizophrenia,[2][3] and appears to be about equal in effectiveness to low-potency antipsychotics like chlorpromazine.[4] It is given by mouth, injection into a muscle, or just under the skin.[2] There is also a long acting injectable version that may last for up to four weeks.[2] Fluphenazine decanoate, the depot injection form of fluphenazine, should not be used by people with severe depression.[5]
Common side effects include movement problems, sleepiness, depression and increased weight.[2] Serious side effects may include neuroleptic malignant syndrome, low white blood cell levels, and the potentially permanent movement disorder tardive dyskinesia.[2] In older people with psychosis as a result of dementia it may increase the risk of dying.[2] It may also increase prolactin levels which may result in milk production, enlarged breasts in males, impotence, and the absence of menstrual periods.[2] It is unclear if it is safe for use in pregnancy.[2] Fluphenazine is a typical antipsychotic of the phenothiazine class.[2] Its mechanism of action is not entirely clear but believed to be related to its ability to block dopamine receptors.[2] In up to 40% of those on long term phenothiazines, liver function tests become mildly abnormal.[6]
Fluphenazine came into use in 1959.[7] The injectable form is on the World Health Organization's List of Essential Medicines.[8] It is available as a generic medication.[2] In the United States the tablets costs between $0.22 and $0.42 per day for a typical dose.[2] The wholesale cost in the developing world of the long acting form is between US$0.20 and US$6.20 per injection as of 2014.[9] It was discontinued in Australia around mid 2017.[10]
Medical use
A 2018 Cochrane review found that fluphenazine's was an imperfect treatment for schizophrenia and other inexpensive medication less associated with side effects may be an equally effective choice.[11]
Dosage
The defined daily dose is 1 mg by injection and 10 mg by mouth.[1] It may be started at doses of 2.5 to 10 mg by mouth divided into three or four times per day.[2] After the person is doing better the dose may be decreased to 1 to 5 mg per day.[2] A formulation that is injected into a muscle may be given at a dose of 12.5 to 25 mg every 4 to 6 weeks.[2]
Side effects
Discontinuation
The British National Formulary recommends a gradual withdrawal when discontinuing antipsychotics to avoid acute withdrawal syndrome or rapid relapse.[12] Symptoms of withdrawal commonly include nausea, vomiting, and loss of appetite.[13] Other symptoms may include restlessness, increased sweating, and trouble sleeping.[13] Less commonly there may be a felling of the world spinning, numbness, or muscle pains.[13] Symptoms generally resolve after a short period of time.[13]
There is tentative evidence that discontinuation of antipsychotics can result in psychosis.[14] It may also result in reoccurrence of the condition that is being treated.[15] Rarely tardive dyskinesia can occur when the medication is stopped.[13]
Pharmacology
Pharmacodynamics
Fluphenazine acts primarily by blocking post-synaptic D2 receptors in the basal ganglia, cortical and limbic system. It also blocks alpha-1 adrenergic receptors, muscarinic-1 receptors, and histamine-1 receptors.[16][17]
Pharmacokinetics
| Medication | Brand name | Class | Vehicle | Dosage | Tmax | t1/2 single | t1/2 multiple | logPc | Ref |
|---|---|---|---|---|---|---|---|---|---|
| Aripiprazole lauroxil | Aristada | Atypical | Watera | 441–1064 mg/4–8 weeks | 24–35 days | ? | 54–57 days | 7.9–10.0 | |
| Aripiprazole monohydrate | Abilify Maintena | Atypical | Watera | 300–400 mg/4 weeks | 7 days | ? | 30–47 days | 4.9–5.2 | |
| Bromperidol decanoate | Impromen Decanoas | Typical | Sesame oil | 40–300 mg/4 weeks | 3–9 days | ? | 21–25 days | 7.9 | [18] |
| Clopentixol decanoate | Sordinol Depot | Typical | Viscoleob | 50–600 mg/1–4 weeks | 4–7 days | ? | 19 days | 9.0 | [19] |
| Flupentixol decanoate | Depixol | Typical | Viscoleob | 10–200 mg/2–4 weeks | 4–10 days | 8 days | 17 days | 7.2–9.2 | [19][20] |
| Fluphenazine decanoate | Prolixin Decanoate | Typical | Sesame oil | 12.5–100 mg/2–5 weeks | 1–2 days | 1–10 days | 14–100 days | 7.2–9.0 | [21][22][23] |
| Fluphenazine enanthate | Prolixin Enanthate | Typical | Sesame oil | 12.5–100 mg/1–4 weeks | 2–3 days | 4 days | ? | 6.4–7.4 | [22] |
| Fluspirilene | Imap, Redeptin | Typical | Watera | 2–12 mg/1 week | 1–8 days | 7 days | ? | 5.2–5.8 | [24] |
| Haloperidol decanoate | Haldol Decanoate | Typical | Sesame oil | 20–400 mg/2–4 weeks | 3–9 days | 18–21 days | 7.2–7.9 | [25][26] | |
| Olanzapine pamoate | Zyprexa Relprevv | Atypical | Watera | 150–405 mg/2–4 weeks | 7 days | ? | 30 days | – | |
| Oxyprothepin decanoate | Meclopin | Typical | ? | ? | ? | ? | ? | 8.5–8.7 | |
| Paliperidone palmitate | Invega Sustenna | Atypical | Watera | 39–819 mg/4–12 weeks | 13–33 days | 25–139 days | ? | 8.1–10.1 | |
| Perphenazine decanoate | Trilafon Dekanoat | Typical | Sesame oil | 50–200 mg/2–4 weeks | ? | ? | 27 days | 8.9 | |
| Perphenazine enanthate | Trilafon Enanthate | Typical | Sesame oil | 25–200 mg/2 weeks | 2–3 days | ? | 4–7 days | 6.4–7.2 | [27] |
| Pipotiazine palmitate | Piportil Longum | Typical | Viscoleob | 25–400 mg/4 weeks | 9–10 days | ? | 14–21 days | 8.5–11.6 | [20] |
| Pipotiazine undecylenate | Piportil Medium | Typical | Sesame oil | 100–200 mg/2 weeks | ? | ? | ? | 8.4 | |
| Risperidone | Risperdal Consta | Atypical | Microspheres | 12.5–75 mg/2 weeks | 21 days | ? | 3–6 days | – | |
| Zuclopentixol acetate | Clopixol Acuphase | Typical | Viscoleob | 50–200 mg/1–3 days | 1–2 days | 1–2 days | 4.7–4.9 | ||
| Zuclopentixol decanoate | Clopixol Depot | Typical | Viscoleob | 50–800 mg/2–4 weeks | 4–9 days | ? | 11–21 days | 7.5–9.0 | |
| Note: All by intramuscular injection. Footnotes: a = Microcrystalline or nanocrystalline aqueous suspension. b = Low-viscosity vegetable oil (specifically fractionated coconut oil with medium-chain triglycerides). c = Predicted, from PubChem and DrugBank. Sources: Main: See template. | |||||||||
History
Fluphenazine came into use in 1959.[7]
Availability
The injectable form is on the World Health Organization's List of Essential Medicines.[8] It is available as a generic medication.[2] In the United States the tablets costs between 0.22 and 0.42 USD per day for a typical dose.[2] The wholesale cost in the developing world of the long acting form is between 0.20 and 6.20 USD per injection as of 2014.[9] It was discontinued in Australia around mid 2017.[10]
Other animals
In horses, it is sometimes given by injection as an anxiety-relieving medication, though there are many negative common side effects and it is forbidden by many equestrian competition organizations.[28]
See also
References
- 1 2 "WHOCC - ATC/DDD Index". www.whocc.no. Archived from the original on 22 January 2021. Retrieved 1 August 2021.
- 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 "fluphenazine decanoate". The American Society of Health-System Pharmacists. Archived from the original on 8 December 2015. Retrieved 1 December 2015.
- ↑ "Product Information: Modecate (Fluphenazine Decanoate Oily Injection )" (PDF). TGA eBusiness Services. Bristol-Myers Squibb Australia Pty Ltd. 1 November 2012. Archived from the original on 2 August 2017. Retrieved 9 December 2013.
- ↑ Tardy M, Huhn M, Engel RR, Leucht S (August 2014). "Fluphenazine versus low-potency first-generation antipsychotic drugs for schizophrenia". The Cochrane Database of Systematic Reviews. 8 (8): CD009230. doi:10.1002/14651858.CD009230.pub2. PMID 25087165.
- ↑ "Modecate Injection 25mg/ml - Patient Information Leaflet (PIL) - (eMC)". www.medicines.org.uk. Archived from the original on 7 November 2017. Retrieved 6 November 2017.
- ↑ "Fluphenazine". livertox.nih.gov. Archived from the original on 17 February 2013. Retrieved 6 November 2017.
- 1 2 McPherson, Edwin M. (2007). Pharmaceutical Manufacturing Encyclopedia (3rd ed.). Burlington: Elsevier. p. 1680. ISBN 9780815518563. Archived from the original on 8 December 2015. Retrieved 2 December 2015.
- 1 2 World Health Organization (2019). World Health Organization model list of essential medicines: 21st list 2019. Geneva: World Health Organization. hdl:10665/325771. WHO/MVP/EMP/IAU/2019.06. License: CC BY-NC-SA 3.0 IGO.
- 1 2 "Fluphenazine Decanoate". International Drug Price Indicator Guide. Archived from the original on 2 August 2017. Retrieved 2 December 2015.
- 1 2 Rossi S, ed. (July 2017). "Fluphenazine - Australian Medicines Handbook". Australian Medicines Handbook. Adelaide, Australia: Australian Medicines Handbook Pty Ltd. Archived from the original on 9 August 2017. Retrieved 8 August 2017.
- ↑ Matar, Hosam E.; Almerie, Muhammad Qutayba; Sampson, Stephanie J. (12 June 2018). "Fluphenazine (oral) versus placebo for schizophrenia". The Cochrane Database of Systematic Reviews. 6: CD006352. doi:10.1002/14651858.CD006352.pub3. ISSN 1469-493X. PMC 6513420. PMID 29893410.
- ↑ Joint Formulary Committee, BMJ, ed. (March 2009). "4.2.1". British National Formulary (57 ed.). United Kingdom: Royal Pharmaceutical Society of Great Britain. p. 192. ISBN 978-0-85369-845-6.
Withdrawal of antipsychotic drugs after long-term therapy should always be gradual and closely monitored to avoid the risk of acute withdrawal syndromes or rapid relapse.
- 1 2 3 4 5 Haddad, Peter; Haddad, Peter M.; Dursun, Serdar; Deakin, Bill (2004). Adverse Syndromes and Psychiatric Drugs: A Clinical Guide. OUP Oxford. pp. 207–216. ISBN 9780198527480. Archived from the original on 22 April 2021. Retrieved 14 July 2019.
- ↑ Moncrieff J (July 2006). "Does antipsychotic withdrawal provoke psychosis? Review of the literature on rapid onset psychosis (supersensitivity psychosis) and withdrawal-related relapse". Acta Psychiatrica Scandinavica. 114 (1): 3–13. doi:10.1111/j.1600-0447.2006.00787.x. PMID 16774655.
- ↑ Sacchetti, Emilio; Vita, Antonio; Siracusano, Alberto; Fleischhacker, Wolfgang (2013). Adherence to Antipsychotics in Schizophrenia. Springer Science & Business Media. p. 85. ISBN 9788847026797. Archived from the original on 22 April 2021. Retrieved 14 July 2019.
- ↑ Siragusa S, Saadabadi A. "Fluphenazine". StatPearls. PMID 29083807. Archived from the original on 28 August 2021. Retrieved 18 April 2020.
- ↑ PubChem. "Fluphenazine". pubchem.ncbi.nlm.nih.gov. Archived from the original on 21 August 2019. Retrieved 30 September 2019.
- ↑ Parent M, Toussaint C, Gilson H (1983). "Long-term treatment of chronic psychotics with bromperidol decanoate: clinical and pharmacokinetic evaluation". Current Therapeutic Research. 34 (1): 1–6.
- 1 2 Jørgensen A, Overø KF (1980). "Clopenthixol and flupenthixol depot preparations in outpatient schizophrenics. III. Serum levels". Acta Psychiatrica Scandinavica. Supplementum. 279: 41–54. doi:10.1111/j.1600-0447.1980.tb07082.x. PMID 6931472.
- 1 2 Reynolds JE (1993). "Anxiolytic sedatives, hypnotics and neuroleptics.". Martindale: The Extra Pharmacopoeia (30th ed.). London: Pharmaceutical Press. pp. 364–623.
- ↑ Ereshefsky L, Saklad SR, Jann MW, Davis CM, Richards A, Seidel DR (May 1984). "Future of depot neuroleptic therapy: pharmacokinetic and pharmacodynamic approaches". The Journal of Clinical Psychiatry. 45 (5 Pt 2): 50–9. PMID 6143748.
- 1 2 Curry SH, Whelpton R, de Schepper PJ, Vranckx S, Schiff AA (April 1979). "Kinetics of fluphenazine after fluphenazine dihydrochloride, enanthate and decanoate administration to man". British Journal of Clinical Pharmacology. 7 (4): 325–31. doi:10.1111/j.1365-2125.1979.tb00941.x. PMC 1429660. PMID 444352.
- ↑ Young D, Ereshefsky L, Saklad SR, Jann MW, Garcia N (1984). Explaining the pharmacokinetics of fluphenazine through computer simulations. (Abstract.). 19th Annual Midyear Clinical Meeting of the American Society of Hospital Pharmacists. Dallas, Texas.
- ↑ Janssen PA, Niemegeers CJ, Schellekens KH, Lenaerts FM, Verbruggen FJ, van Nueten JM, et al. (November 1970). "The pharmacology of fluspirilene (R 6218), a potent, long-acting and injectable neuroleptic drug". Arzneimittel-Forschung. 20 (11): 1689–98. PMID 4992598.
- ↑ Beresford R, Ward A (January 1987). "Haloperidol decanoate. A preliminary review of its pharmacodynamic and pharmacokinetic properties and therapeutic use in psychosis". Drugs. 33 (1): 31–49. doi:10.2165/00003495-198733010-00002. PMID 3545764.
- ↑ Reyntigens AJ, Heykants JJ, Woestenborghs RJ, Gelders YG, Aerts TJ (1982). "Pharmacokinetics of haloperidol decanoate. A 2-year follow-up". International Pharmacopsychiatry. 17 (4): 238–46. doi:10.1159/000468580. PMID 7185768.
- ↑ Larsson M, Axelsson R, Forsman A (1984). "On the pharmacokinetics of perphenazine: a clinical study of perphenazine enanthate and decanoate". Current Therapeutic Research. 36 (6): 1071–88.
- ↑ Loving NS (31 March 2012). "Effects of Behavior-Modifying Drug Investigated (AAEP 2011)". The Horse Media Group. Archived from the original on 6 January 2017. Retrieved 13 December 2016.
External links
| External sites: |
|
|---|---|
| Identifiers: |