Recreational drug use
Recreational drug use indicates the use of one or more psychoactive drugs to induce an altered state of consciousness either for pleasure or for some other casual purpose or pastime by modifying the perceptions, feelings, and emotions of the user.[1] When a psychoactive drug enters the user's body, it induces an intoxicating effect.[1] Generally, recreational drugs are divided into three categories: depressants (drugs that induce a feeling of relaxation and calmness); stimulants (drugs that induce a sense of energy and alertness); and hallucinogens (drugs that induce perceptual distortions such as hallucination).[2]

In popular practice, recreational drug use generally is a tolerated social behaviour,[1] rather than perceived as the medical condition of self-medication.[3] However, heavy use of some drugs is socially stigmatized.[4] Many people also use prescribed and controlled depressants such as opioids, as well as opiates and benzodiazepines.[2]
Common recreational drugs include caffeine, commonly found in coffee, tea, soft drinks, chocolate, prescription drugs; alcohol, commonly found in beer, wine, and distilled spirits; nicotine, commonly found in tobacco and electronic cigarettes; cannabis and hashish (with legality of possession varying inter/intra-nationally); and the controlled substances listed as controlled drugs in the Single Convention on Narcotic Drugs (1961) and the Convention on Psychotropic Substances (1971) of the United Nations. What controlled substances are considered generally unlawful to possess varies by country, but usually includes cannabis, cocaine, opiates, MDMA, amphetamine, methamphetamine, LSD, psilocybin, mescaline, and benzodiazepines. In 2015, it was estimated that about 5% of people worldwide aged 15 to 65 (158 million to 351 million) had used controlled drugs at least once.[5]
Reasons for use
.jpg.webp)
Many researchers have explored the etiology of recreational drug use.[1] Some of the most common theories are: genetics, personality type, psychological problems, self-medication, sex, age, instant gratification, basic human need, curiosity, rebelliousness, a sense of belonging to a group, family and attachment issues, history of trauma, failure at school or work, socioeconomic stressors, peer pressure, juvenile delinquency, availability, historical factors, or socio-cultural influences.[7][8] There has not been agreement around any one single cause.[7] Instead, experts tend to apply the biopsychosocial model.[7] Any number of these factors are likely to influence an individual's drug use as they are not mutually exclusive.[7][8][9] Regardless of genetics, mental health, or traumatic experiences, social factors play a large role in exposure to and availability of certain types of drugs and patterns of drug use.[7][8][10]
According to addiction researcher Martin A. Plant, many people go through a period of self-redefinition before initiating recreational drug use.[8] They tend to view using drugs as part of a general lifestyle that involves belonging to a subculture that they associate with heightened status and the challenging of social norms.[8] Plant states: "From the user's point of view there are many positive reasons to become part of the milieu of drug taking. The reasons for drug use appear to have as much to do with needs for friendship, pleasure and status as they do with unhappiness or poverty. Becoming a drug taker, to many people, is a positive affirmation rather than a negative experience".[8]
Evolution
Anthropological research has suggested that humans "may have evolved to counter-exploit plant neurotoxins". The ability to use botanical chemicals to serve the function of endogenous neurotransmitters may have improved survival rates, conferring an evolutionary advantage. A typically restrictive prehistoric diet may have emphasised the apparent benefit of consuming psychoactive drugs, which had themselves evolved to imitate neurotransmitters.[11] Chemical–ecological adaptations, and the genetics of hepatic enzymes, particularly cytochrome P450, have led researchers to propose that "humans have shared a co-evolutionary relationship with psychotropic plant substances that is millions of years old."[12]
Health risks
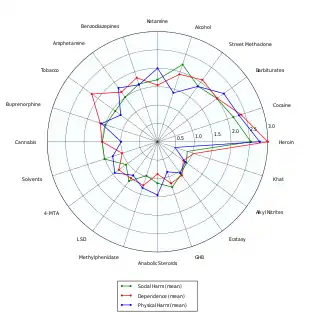

Severity and type of risks that come with recreational drug use vary widely with the drug in question and the amount being used. There are many factors in the environment and within the user that interact with each drug differently. Overall, some studies suggest that alcohol is one of the most dangerous of all recreational drugs; only heroin, crack cocaine, and methamphetamine are judged to be more harmful. Alcoholic drinks, tobacco products and other nicotine-based products (e.g., electronic cigarettes), and cannabis are regarded by various medical professionals to be the most common and widespread gateway drugs.[14][15][16][17] In the United States, Australia, and New Zealand, the general onset of drinking alcohol, tobacco smoking, cannabis smoking, and consumption of multiple drugs among young people most frequently occurs during adolescence and within school settings (middle school and secondary school).[16][17][18][19][20]
Scientific studies which focus on a low–moderate level of alcohol consumption, particularly of red wine,[21][22][23] have concluded that there can be substantial health benefits from its use, such as decreased risk of cardiovascular diseases, stroke, and cognitive decline.[21][22][23][24] This claim has been disputed.[21] Researcher David Nutt stated that these studies showing benefits for "moderate" alcohol consumption lacked control for the variable of what the subjects were drinking, beforehand.[25] Experts in the United Kingdom have suggested that some psychoactive drugs that may be causing less harm to fewer users (although they are also used less frequently in the first place) include cannabis, psilocybin mushrooms, LSD, and MDMA. However, these drugs are not without their own particular risks and side effects.[26]
Drug harmfulness

Drug harmfulness is defined as the degree to which a psychoactive drug is harmful to a user and is measured in various ways, such as by addictiveness and the potential for physical harm. More harmful drugs are called "hard drugs",[27] and less harmful drugs are called "soft drugs".[28] The term "soft drug" is considered controversial by its critics as it may imply that soft drugs cause no or insignificant harm.[28]

Responsible use
The concept of "responsible drug use" is that a person can use drugs recreationally or otherwise with reduced or eliminated risk of negatively affecting other aspects of one's life or other people's lives. Advocates of this philosophy point to the many well-known artists and intellectuals who have used drugs, experimentally or otherwise, with few detrimental effects on their lives. Responsible drug use becomes problematic only when the use of the substance significantly interferes with the user's daily life.
Responsible drug use advocates that users should not take drugs at the same time as activities such as driving, swimming, operating machinery, or other activities that are unsafe without a sober state. Responsible drug use is emphasized as a primary prevention technique in harm-reduction drug policies. Harm-reduction policies were popularized in the late 1980s, although they began in the 1970s counter-culture, when cartoons explaining responsible drug use and the consequences of irresponsible drug use were distributed to users.[31] Another issue is that the illegality of drugs in itself also causes social and economic consequences for those using them—the drugs may be "cut" with adulterants and the purity varies wildly, making overdoses more likely—and legalization of drug production and distribution would reduce these and other dangers of illegal drug use.[32] Harm reduction seeks to minimize the harm that can occur through the use of various drugs, whether legal (e.g., alcohol and nicotine), or illegal (e.g., heroin and cocaine). For example, people who take drugs intravenously (cocaine, heroin) can minimize harm to both themselves and members of the community through proper injecting technique, using new needles and syringes each time, and proper disposal of all injecting equipment.
Prevention
In efforts to curtail recreational drug use, governments worldwide introduced several laws prohibiting the possession of almost all varieties of recreational drugs during the 20th century. The West's "War on Drugs" however, is now facing increasing criticism. Evidence is insufficient to tell if behavioral interventions help prevent recreational drug use in children.[33]
One in four adolescents has used an illegal drug and one in ten of those adolescents who need addiction treatment get some type of care.[34] School-based programs are the most commonly used method for drug use education; however, the success rates of these intervention programs is highly dependent on the commitment of participants, and is limited in general.[35] Studies have also shown that home intervention is also effective in decreasing the appeal of drugs.
Demographics

Australia
Alcohol is the most widely used drug in Australia.[38] 86.2% of Australians aged 12 years and over have consumed alcohol at least once in their lifetime, compared to 34.8% of Australians aged 12 years and over who have used cannabis at least once in their lifetime.[38]
United States
From the mid-19th century to the 1930s, American physicians prescribed Cannabis sativa as a prescription drug for various medical conditions.[39] In the 1960s, the counterculture movement introduced the use of psychoactive drugs, including cannabis. Young adults and college students reported the recreational prevalence of cannabis, among other drugs, at 20-25% while the cultural mindset of using was open and curious.[40] In 1969, the FBI reported that between the years 1966 and 1968, the number of arrests for marijuana possession, which had been outlawed throughout the United States under Marijuana Tax Act of 1937, had increased by 98%.[41] Despite acknowledgement that drug use was greatly growing among America's youth during the late 1960s, surveys have suggested that only as much as 4% of the American population had ever smoked marijuana by 1969. By 1972, however, that number would increase to 12%. That number would then double by 1977.[42]
The Controlled Substances Act of 1970 classified marijuana along with heroin and LSD as a Schedule I drug, i.e., having the relatively highest abuse potential and no accepted medical use.[39][43] Most marijuana at that time came from Mexico, but in 1975 the Mexican government agreed to eradicate the crop by spraying it with the herbicide paraquat, raising fears of toxic side effects. Colombia then became the main supplier.[43] The "zero tolerance" climate of the Reagan and Bush administrations (1981–93) resulted in passage of strict laws and mandatory sentences for possession of marijuana. The "War on Drugs" thus brought with it a shift from reliance on imported supplies to domestic cultivation (particularly in Hawaii and California). Beginning in 1982, the Drug Enforcement Administration turned increased attention to marijuana farms in the United States, and there was a shift to the indoor growing of plants specially developed for small size and high yield. After over a decade of decreasing use, marijuana smoking began an upward trend once more in the early 1990s, especially among teenagers, but by the end of the decade this upswing had leveled off well below former peaks of use.[43]
Society and culture

Many movements and organizations are advocating for or against the liberalization of the use of recreational drugs, most notably regarding the legalization of marijuana and cannabinoids for medical and/or recreational use.[39][44][45][46] Subcultures have emerged among users of recreational drugs,[47] as well as alternative lifestyles and social movements among those who abstain from them, such as teetotalism and "straight edge".[48]
Since the early 2000s, medical professionals have acknowledged and addressed the problem of the increasing consumption of alcoholic drinks and club drugs (such as MDMA, cocaine, rohypnol, GHB, ketamine, PCP, LSD, and methamphetamine) associated with rave culture among adolescents and young adults in the Western world.[49][50][51][52][53] Studies have shown that adolescents are more likely than young adults to use multiple drugs,[54] and the consumption of club drugs is highly associated with the presence of criminal behaviors and recent alcohol abuse or dependence.[55]
The prevalence of recreational drugs in human societies is widely reflected in fiction, entertainment, and the arts, subject to prevailing laws and social conventions. For instance, in the music industry, the musical genres hip hop, hardcore rap, and trap, alongside their derivative subgenres and subcultures, are most notorious for having continuously celebrated and promoted drug trafficking, gangster lifestyle, and consumption of drugs and alcohol since their inception in the United States during the late 1980s–early 1990s.[56][57][58][59] In video games, for example, drugs are portrayed in a variety of ways: including power-ups (cocaine gum replenishes stamina in Red Dead Redemption 2), obstacles to be avoided (such as the Fuzzies in Super Mario World 2: Yoshi's Island that distort the player's view when accidentally consumed), items to be bought and sold for in-game currency (coke dealing is a big part of Scarface: The World Is Yours). In 1997's Fallout, drugs ("chems" in the game) can fill the role of any above mentioned. Drug trafficking, gang rivalries, and their related criminal underworld also play a big part in the best-selling Grand Theft Auto video game franchise.
Common recreational drugs
The following substances are commonly used recreationally:[60]
- Alcohol: Most drinking alcohol is ethanol, CH
3CH
2OH. Drinking alcohol creates intoxication, relaxation and lowered inhibitions. It is produced by the fermentation of sugars by yeasts to create wine, beer, and distilled liquor (e.g., vodka, rum, gin, etc.). In most areas of the world, it is legal for those over a certain age (18 in most countries). It is an IARC Group 1 carcinogen and a teratogen.[61] Alcohol withdrawal can be life-threatening.[62] - Amphetamines: Used recreationally to provide alertness and a sense of energy. Prescribed for ADHD, narcolepsy, depression and weight loss. A potent central nervous system stimulant, in the 1940s and 50s methamphetamine was used by Axis and Allied troops in World War II, and, later on, other armies, and by Japanese factory workers. It increases muscle strength and fatigue resistance and improves reaction time.[63] Methamphetamine use can be neurotoxic, which means it damages dopamine neurons.[64] As a result of this brain damage, chronic use can lead to post acute withdrawal syndrome.[65]
- Caffeine: Often found in coffee, black tea, energy drinks, some soft drinks (e.g., Coca-Cola, Pepsi and Mountain Dew, among others), and chocolate. It is the world's most widely consumed psychoactive drug, but has only mild dependence liability for long-term users.[66]
- Cannabis: Its common forms include marijuana and hashish, which are smoked, vaporized or eaten. It contains at least 85 cannabinoids. The primary psychoactive component is THC, which mimics the neurotransmitter anandamide, named after the Hindu ananda, "joy, bliss, delight". When cannabis is eaten, THC metabolized into 11-OH-THC, this molecule is the primary psychoactive coumpound of edible forms of cannabis. THC and 11-OH-THC are partial agonist at CB1 and CB2 receptors of the endocannabinoid system.
- Cocaine: It is available as a white powder, which is insufflated ("sniffed" into the nostrils) or converted into a solution with water and injected. A popular derivative, crack cocaine is typically smoked. When transformed into its freebase form, crack, the cocaine vapour may be inhaled directly. This is thought to increase bioavailability, but has also been found to be toxic, due to the production of methylecgonidine during pyrolysis.[67][68][69]
- MDMA: Commonly known as ecstasy, it is a common club drug in the rave scene.
- Electronic cigarette: A large proportion of e-cigarette use is recreational.[70] Most e-cigarette liquids contain nicotine, but the level of nicotine varies depending on user-preference and manufacturers.[71] Nicotine is highly addictive,[72][73][74] comparable to heroin or cocaine.[75] E-cigarettes are being used to inhale MDMA, cocaine powder, crack cocaine, synthetic cathinones, mephedrone, α-PVP, synthetic cannabinoids, opioids, heroin, fentanyl, tryptamines, and ketamine.[76]
- Ketamine: An anesthetic used legally by paramedics and doctors in emergency situations for its dissociative and analgesic qualities and illegally in the club drug scene.
- Lean: A liquid drug mixture made when mixing cough syrup, sweets, soft drinks and codeine. It originated in the 1990s in Houston. Ever since then, this drug usage has grown and is often used at parties and in the trap music scene. Many people would get a drowsy feeling when consuming this drug.
- LSD: A popular ergoline derivative, that was first synthesized in 1938 by Albert Hofmann. However, he failed to notice its psychedelic effects until 1943.[77] It's a serotonergic psychedelic (partial agonist at serotonin receptors, particularly the 5-HT2A subtypes) like psilocin, mescaline and DMT. But LSD is unique because it is also a partial agonist of dopamine and norepinephrine receptors, particularly the D2R subtypes. LSD (d-Lysergic Acid Diethylamide) is a molecule of the lysergamide family, a subclass of the tryptamine family. In the 1950s, it was used in psychological therapy, and, covertly, by the CIA in Project MKULTRA, in which the drug was administered to unwitting US and Canadian citizens. It played a central role in 1960s 'counter-culture', and was banned in October 1968 by US President Lyndon B Johnson.[78][79]
- Nitrous oxide: legally used by dentists as an anxiolytic and anaesthetic, it is also used recreationally by users who obtain it from whipped cream canisters (whippets or whip-its) (see inhalant), as it causes perceptual effects, a "high" and at higher doses, hallucinations.
- Opiates and opioids: Available by prescription for pain relief. Commonly used opioids include oxycodone, hydrocodone, codeine, fentanyl, heroin, methadone, and morphine. Opioids have a high potential for addiction and have the ability to induce severe physical withdrawal symptoms upon cessation of frequent use. Heroin can be smoked, insufflated or turned into a solution with water and injected. Percocet is a prescription opioid containing oxycodone and acetaminophen.
- Psilocybin mushrooms: This hallucinogenic drug was an important drug in the psychedelic scene. Until 1963, when it was chemically analysed by Albert Hofmann, it was completely unknown to modern science that Psilocybe semilanceata ("Liberty Cap", common throughout Europe) contains psilocybin, a hallucinogen previously identified only in species native to Mexico, Asia, and North America.[80]
- Tobacco: Nicotiana tabacum. Nicotine is the key drug contained in tobacco leaves, which are either smoked, chewed or snuffed. It contains nicotine, which crosses the blood–brain barrier in 10–20 seconds. It mimics the action of the neurotransmitter acetylcholine at nicotinic acetylcholine receptors in the brain and the neuromuscular junction. The neuronal forms of the receptor are present both post-synaptically (involved in classical neurotransmission) and pre-synaptically, where they can influence the release of multiple neurotransmitters.[81]
- Tranquilizers: barbiturates, benzodiazepines (e.g. alprazolam, diazepam, etc.)(commonly prescribed for anxiety disorders; known to cause dementia and post acute withdrawal syndrome)
- "Bath salts": slang term that generally refers to substituted cathinones such as Mephedrone and Methylenedioxypyrovalerone (MDPV), but not always
- DMT – primary ingredient in ayahuasca, can also be smoked (inhalation causes a brief effect lasting usually 5 to 15 minutes).[82][83]
- Peyote: This hallucinogen contains mescaline, native to southwestern Texas and Mexico
- Salvia divinorum: This hallucinogenic Mexican herb in the mint family; not considered recreational, most likely due to the nature of the hallucinations (legal in some jurisdictions)
- Synthetic cannabis: "Spice", "K2", JWH-018, AM-2201
- Quaaludes: A popular club drug in the 1970s. No longer prescribed or manufactured in many countries but remains popular in South Africa.[84][85]
Routes of administration


Drugs are often associated with a particular route of administration. Many drugs can be consumed in more than one way. For example, marijuana can be swallowed like food or smoked, and cocaine can be "sniffed" in the nostrils, injected, or, with various modifications, smoked.
- inhalation: all intoxicative inhalants (see below) that are gases or solvent vapours that are inhaled through the trachea, as the name suggests
- insufflation: also known as "snorting", or "sniffing", this method involves the user placing a powder in the nostrils and breathing in through the nose, so that the drug is absorbed by the mucous membranes. Drugs that are "snorted", or "sniffed", include powdered amphetamines, cocaine, heroin, ketamine, MDMA, snuff tobacco
- Subcutaneous injection: also known as Skin popping. Injection of drug into the third lowest layer of skin.
- Intramuscular injection: injection of drug into a muscle.
- intravenous injection (see also the article Drug injection): the user injects a solution of water and the drug into a vein, or less commonly, into the tissue. Drugs that are injected include morphine and heroin, less commonly other opioids. Stimulants like cocaine or methamphetamine may also be injected. In rare cases, users inject other drugs.
- oral intake: caffeine, ethanol, cannabis edibles, psilocybin mushrooms, coca tea, poppy tea, laudanum, GHB, ecstasy pills with MDMA or various other substances (mainly stimulants and psychedelics), prescription and over-the-counter drugs (ADHD and narcolepsy medications, benzodiazepines, anxiolytics, sedatives, cough suppressants, morphine, codeine, opioids and others)
- sublingual: substances diffuse into the blood through tissues under the tongue. Many psychoactive drugs can be or have been specifically designed for sublingual administration, including barbiturates, benzodiazepines,[86] opioid analgesics with poor gastrointestinal bioavailability, LSD blotters, coca leaves, some hallucinogens. This route of administration is activated when chewing some forms of smokeless tobacco (e.g. dipping tobacco, snus).
- intrarectal: administering into the rectum, most water-soluble drugs can be used this way.
- smoking (see also the section below): tobacco, cannabis, opium, crystal meth, phencyclidine, crack cocaine and heroin (diamorphine as freebase) known as chasing the dragon.
- transdermal patches with prescription drugs: e.g. methylphenidate (Daytrana) and fentanyl.[87][88][89][90]
Many drugs are taken through various routes. Intravenous route is the most efficient, but also one of the most dangerous. Nasal, rectal, inhalation and smoking are safer. The oral route is one of the safest and most comfortable, but of little bioavailability.
Types
Depressants
Depressants are psychoactive drugs that temporarily diminish the function or activity of a specific part of the body or mind.[91] Colloquially, depressants are known as "downers", and users generally take them to feel more relaxed and less tense. Examples of these kinds of effects may include anxiolysis, sedation, and hypotension. Depressants are widely used throughout the world as prescription medicines and as illicit substances. When these are used, effects may include anxiolysis (reduction of anxiety), analgesia (pain relief), sedation, somnolence, cognitive/memory impairment, dissociation, muscle relaxation, lowered blood pressure/heart rate, respiratory depression, anesthesia, and anticonvulsant effects. Depressants exert their effects through a number of different pharmacological mechanisms, the most prominent of which include potentiation of GABA or opioid activity, and inhibition of adrenergic, histamine or acetylcholine activity. Some are also capable of inducing feelings of euphoria. The most widely used depressant by far is alcohol (i.e. ethanol).
Stimulants or "uppers", such as amphetamines or cocaine, which increase mental or physical function, have an opposite effect to depressants.
Depressants, in particular alcohol, can precipitate psychosis. A 2019 systematic review and meta-analysis by Murrie et al. found that the rate of transition from opioid, alcohol and sedative induced psychosis to schizophrenia was 12%, 10% and 9% respectively.[92]
Antihistamines
Antihistamines (or "histamine antagonists") inhibit the release or action of histamine. "Antihistamine" can be used to describe any histamine antagonist, but the term is usually reserved for the classical antihistamines that act upon the H1 histamine receptor. Antihistamines are used as treatment for allergies. Allergies are caused by an excessive response of the body to allergens, such as the pollen released by grasses and trees. An allergic reaction causes release of histamine by the body. Other uses of antihistamines are to help with normal symptoms of insect stings even if there is no allergic reaction. Their recreational appeal exists mainly due to their anticholinergic properties, that induce anxiolysis and, in some cases such as diphenhydramine, chlorpheniramine, and orphenadrine, a characteristic euphoria at moderate doses. High dosages taken to induce recreational drug effects may lead to overdoses. Antihistamines are also consumed in combination with alcohol, particularly by youth who find it hard to obtain alcohol. The combination of the two drugs can cause intoxication with lower alcohol doses.
Hallucinations and possibly delirium resembling the effects of Datura stramonium can result if the drug is taken in much higher than therapeutic doses. Antihistamines are widely available over the counter at drug stores (without a prescription), in the form of allergy medication and some cough medicines. They are sometimes used in combination with other substances such as alcohol. The most common unsupervised use of antihistamines in terms of volume and percentage of the total is perhaps in parallel to the medicinal use of some antihistamines to extend and intensify the effects of opioids and depressants. The most commonly used are hydroxyzine, mainly to extend a supply of other drugs, as in medical use, and the above-mentioned ethanolamine and alkylamine-class first-generation antihistamines, which are – once again as in the 1950s – the subject of medical research into their anti-depressant properties.
For all of the above reasons, the use of medicinal scopolamine for recreational uses is also observed.
Analgesics
Analgesics (also known as "painkillers") are used to relieve pain (achieve analgesia). The word analgesic derives from Greek "αν-" (an-, "without") and "άλγος" (álgos, "pain"). Analgesic drugs act in various ways on the peripheral and central nervous systems; they include paracetamol (also known in the US as acetaminophen), the nonsteroidal anti-inflammatory drugs (NSAIDs) such as the salicylates (e.g. aspirin), and opioid drugs such as hydrocodone, codeine, heroin and oxycodone. Some further examples of the brand name prescription opiates and opioid analgesics that may be used recreationally include Vicodin, Lortab, Norco (hydrocodone), Avinza, Kapanol (morphine), Opana, Paramorphan (oxymorphone), Dilaudid, Palladone (hydromorphone), and OxyContin (oxycodone).
Tranquilizers
The following are examples of tranquilizers (GABAergics):
- Barbiturates
- Benzodiazepines
- Ethanol (drinking alcohol; ethyl alcohol)
- Nonbenzodiazepines
- Others
- carisoprodol (Soma)
- chloral hydrate
- diethyl ether
- ethchlorvynol (Placidyl; "jelly-bellies")
- gamma-butyrolactone (GBL, a prodrug to GHB)
- gamma-hydroxybutyrate (GHB; G; Xyrem; "Liquid Ecstasy", "Fantasy")
- glutethimide (Doriden)
- kava (from Piper methysticum; contains kavalactones)
- ketamine, a phencyclidine (PCP) analog
- meprobamate (Miltown)
- methaqualone (Sopor, Mandrax; "Quaaludes")
- phenibut
- propofol (Diprivan), a general anesthetic
- theanine (found in Camellia sinensis, the tea plant)
- valerian (from Valeriana officinalis)
Stimulants

Stimulants, also known as "psychostimulants",[93] induce euphoria with improvements in mental and physical function, such as enhanced alertness, wakefulness, and locomotion. Stimulants are also occasionally called "uppers". Depressants or "downers", which decrease mental or physical function, are in stark contrast to stimulants and are considered to be their functional opposites.
Stimulants enhance the activity of the central and peripheral nervous systems. Common effects may include increased alertness, awareness, wakefulness, endurance, productivity, and motivation, arousal, locomotion, heart rate, and blood pressure, and a diminished desire for food and sleep.
Use of stimulants may cause the body to significantly reduce its production of endogenous compounds that fulfill similar functions. Once the effect of the ingested stimulant has worn off the user may feel depressed, lethargic, confused, and dysphoric. This is colloquially termed a "crash" and may promote reuse of the stimulant.
Amphetamines are a significant cause of drug-induced psychosis. Importantly, a 2019 meta-analysis found that 22% of people with amphetamine-induced psychosis transition to a later diagnosis of schizophrenia.[92]
Examples of stimulants include:
- Sympathomimetics (catecholaminergics)—e.g. amphetamine, methamphetamine, cocaine, methylphenidate, ephedrine, pseudoephedrine
- Entactogens (serotonergics, primarily phenethylamines)—e.g. MDMA (which is also an amphetamine)
- Eugeroics, e.g. modafinil
- Others
- arecoline (found in Areca catechu)
- caffeine (found in Coffea spp.)
- nicotine (found in Nicotiana spp.)
- rauwolscine (found in Rauvolfia serpentina)
- yohimbine (Procomil; a tryptamine alkaloid found in Pausinystalia johimbe)
Euphoriants
- Alcohol: "Euphoria, the feeling of well-being, has been reported during the early (10–15 min) phase of alcohol consumption" (e.g., beer, wine or spirits)[94]
- Cannabis: Tetrahydrocannabinol, the main psychoactive ingredient in this plant, can have sedative and euphoric properties.
- Catnip: Catnip contains a sedative known as nepetalactone that activates opioid receptors. In cats it elicits sniffing, licking, chewing, head shaking, rolling, and rubbing which are indicators of pleasure. In humans, however, catnip does not act as a euphoriant.[95]
- Stimulants: "Psychomotor stimulants produce locomotor activity (the subject becomes hyperactive), euphoria, (often expressed by excessive talking and garrulous behaviour), and anorexia. The amphetamines are the best known drugs in this category..."[96]
- MDMA: The "euphoriant drugs such as MDMA ('ecstasy') and MDEA ('eve')" are popular among young adults.[97] MDMA "users experience short-term feelings of euphoria, rushes of energy and increased tactility"[98] as well as interpersonal connectedness.
- Opium: This "drug derived from the unripe seed-pods of the opium poppy…produces drowsiness and euphoria and reduces pain. Morphine and codeine are opium derivatives."[99] Opioids have led to many deaths in the United States, particularly by causing respiratory depression.
Hallucinogens
Hallucinogens can be divided into three broad categories: psychedelics, dissociatives, and deliriants. They can cause subjective changes in perception, thought, emotion and consciousness. Unlike other psychoactive drugs such as stimulants and opioids, hallucinogens do not merely amplify familiar states of mind but also induce experiences that differ from those of ordinary consciousness, often compared to non-ordinary forms of consciousness such as trance, meditation, conversion experiences, and dreams.
Psychedelics, dissociatives, and deliriants have a long worldwide history of use within medicinal and religious traditions. They are used in shamanic forms of ritual healing and divination, in initiation rites, and in the religious rituals of syncretistic movements such as União do Vegetal, Santo Daime, Temple of the True Inner Light, and the Native American Church. When used in religious practice, psychedelic drugs, as well as other substances like tobacco, are referred to as entheogens.
Hallucinogen-induced psychosis occurs when psychosis persists despite no longer being intoxicated with the drug. It is estimated that 26% of people with hallucinogen-induced psychosis will transition to a diagnosis of schizophrenia. This percentage is less than the psychosis transition rate for cannabis (34%) but higher than that of amphetamines (22%).[92]
Starting in the mid-20th century, psychedelic drugs have been the object of extensive attention in the Western world. They have been and are being explored as potential therapeutic agents in treating depression, post-traumatic stress disorder, obsessive-compulsive disorder, alcoholism, and opioid addiction. Yet the most popular, and at the same time most stigmatized, use of psychedelics in Western culture has been associated with the search for direct religious experience, enhanced creativity, personal development, and "mind expansion". The use of psychedelic drugs was a major element of the 1960s counterculture, where it became associated with various social movements and a general atmosphere of rebellion and strife between generations.
- Deliriants
- atropine (alkaloid found in plants of the family Solanaceae, including datura, deadly nightshade, henbane and mandrake)
- dimenhydrinate (Dramamine, an antihistamine)
- diphenhydramine (Benadryl, Unisom, Nytol)
- hyoscyamine (alkaloid also found in the Solanaceae)
- hyoscine hydrobromide (another Solanaceae alkaloid)
- myristicin (found in Myristica fragrans ("Nutmeg"))
- ibotenic acid (found in Amanita muscaria ("Fly Agaric"); prodrug to muscimol)
- muscimol (also found in Amanita muscaria, a GABAergic)
- Dissociatives
- dextromethorphan (DXM; Robitussin, Delsym, etc.; "Dex", "Robo", "Cough Syrup", "DXM")
- "Triple C's, Coricidin, Skittles" refer to a potentially fatal formulation containing both dextromethorphan and chlorpheniramine.
- ketamine (K; Ketalar, Ketaset, Ketanest; "Ket", "Kit Kat", "Special-K", "Vitamin K", "Jet Fuel", "Horse Tranquilizer")
- methoxetamine (Mex, Mket, Mexi)
- phencyclidine (PCP; Sernyl; "Angel Dust", "Rocket Fuel", "Sherm", "Killer Weed", "Super Grass")
- nitrous oxide (N2O; "NOS", "Laughing Gas", "Whippets", "Balloons")
- dextromethorphan (DXM; Robitussin, Delsym, etc.; "Dex", "Robo", "Cough Syrup", "DXM")
- Psychedelics
- Phenethylamines
- 2C-B ("Nexus", "Venus", "Eros", "Bees")
- 2C-E ("Eternity", "Hummingbird")
- 2C-I ("Infinity")
- 2C-T-2 ("Rosy")
- 2C-T-7 ("Blue Mystic", "Lucky 7")
- DOB
- DOC
- DOI
- DOM ("Serenity, Tranquility, and Peace" ("STP"))
- MDMA ("Ecstasy", "E", "Molly", "Mandy", "MD", "Crystal Love")
- mescaline (found in peyote, Peruvian torch cactus and San Pedro cactus)
- Tryptamines (including ergolines and lysergamides)
- 5-MeO-DiPT ("Foxy", "Foxy Methoxy")
- 5-MeO-DMT (found in various plants like chacruna, jurema, vilca, and yopo)
- alpha-methyltryptamine (αMT; Indopan; "Spirals")
- bufotenin (secreted by Bufo alvarius, also found in various Amanita mushrooms)
- N,N-dimethyltryptamine (N,N-DMT; DMT; "Dimitri", "Disneyland", "Spice"; found in large amounts in Psychotria and in D. cabrerana)
- lysergic acid amide (LSA; ergine; found in morning glory and Hawaiian baby woodrose seeds)
- lysergic acid diethylamide (LSD; L; Delysid; "Acid", "Sid". "Cid", "Lucy", "Sidney", "Blotters", "Droppers", "Sugar Cubes")
- O-Acetylpsilocin (believed to be a prodrug of psilocin)
- psilocin (found in psilocybin mushrooms)
- psilocybin (also found in psilocybin mushrooms; prodrug to psilocin)
- ibogaine (found in Tabernanthe iboga ("Iboga"))
- Phenethylamines
- Atypicals
- salvinorin A (found in Salvia divinorum, a trans-neoclerodane diterpenoid ("Diviner's Sage", "Lady Salvia", "Salvinorin"))
- tetrahydrocannabinol (found in cannabis)
Inhalants
Inhalants are gases, aerosols, or solvents that are breathed in and absorbed through the lungs. While some "inhalant" drugs are used for medical purposes, as in the case of nitrous oxide, a dental anesthetic, inhalants are used as recreational drugs for their intoxicating effect.[100] Most inhalant drugs that are used non-medically are ingredients in household or industrial chemical products that are not intended to be concentrated and inhaled, including organic solvents (found in cleaning products, fast-drying glues, and nail polish removers), fuels (gasoline (petrol) and kerosene), and propellant gases such as Freon and compressed hydrofluorocarbons that are used in aerosol cans such as hairspray, whipped cream, and non-stick cooking spray. A small number of recreational inhalant drugs are pharmaceutical products that are used illicitly, such as anesthetics (ether and nitrous oxide)[100] and volatile anti-angina drugs (alkyl nitrites, more commonly known as "poppers").
The most serious inhalant abuse occurs among children and teens who "[...] live on the streets completely without family ties".[101] Inhalant users inhale vapor or aerosol propellant gases using plastic bags held over the mouth or by breathing from a solvent-soaked rag or an open container. The effects of inhalants range from an alcohol-like intoxication and intense euphoria to vivid hallucinations, depending on the substance and the dosage. Some inhalant users are injured due to the harmful effects of the solvents or gases, or due to other chemicals used in the products inhaled. As with any recreational drug, users can be injured due to dangerous behavior while they are intoxicated, such as driving under the influence. Computer cleaning dusters are dangerous to inhale, because the gases expand and cool rapidly upon being sprayed. In many cases, users have died from hypoxia (lack of oxygen), pneumonia, cardiac failure or arrest,[102] or aspiration of vomit.
Examples include:
- Chloroform
- Ethyl chloride
- Diethyl ether
- Ethane and ethylene
- Laughing gas (nitrous oxide)[100]
- Poppers (alkyl nitrites)
- Solvents and propellants (including propane, butane, freon, gasoline, kerosene, toluene) along with the fumes of glues containing them
List of drugs which can be smoked
Plants:
- tobacco
- cannabis
- salvia divinorum
- opium
- datura and other Solanaceae (formerly smoked to treat asthma)
- possibly other plants (see the section below)
Substances (also not necessarily psychoactive plants smoked within them):
- methamphetamine
- crack cocaine
- black tar heroin
- phencyclidine (PCP)
- synthetic cannabinoids (see also: synthetic cannabis)
- dimethyltryptamine (DMT)
- 5-MeO-DMT
- Bufotenine
- DiPT
- Methaqualone
- Ethanol (alcohol)
- Ketamine
- Heroin
- many others, including some prescription drugs
List of psychoactive plants, fungi, and animals
Minimally psychoactive plants which contain mainly caffeine and theobromine:
- coffee
- tea (caffeine in tea is sometimes called theine) – also contains theanine
- guarana (caffeine in guarana is sometimes called guaranine)
- yerba mate (caffeine in yerba mate is sometimes called mateine)
- cocoa
- kola
Most known psychoactive plants:
- cannabis: cannabinoids
- tobacco: nicotine and beta-carboline alkaloids
- coca: cocaine
- opium poppy: morphine, codeine, and other opiates
- salvia divinorum: salvinorin A
- khat: cathine and cathinone
- kava: kavalactones
- nutmeg: myristicin and elemicin
Solanaceae plants—contain atropine, hyoscyamine, and scopolamine
- datura
- deadly nightshade Atropa belladonna
- henbane
- mandrake (mandragora)
- other Solanaceae
Cacti with mescaline:
- peyote
- Peruvian torch cactus
- San Pedro cactus
Other plants:
- kratom: mitragynine, mitraphylline, 7-hydroxymitragynine, raubasine, and corynanthine
- ephedra: ephedrine
- damiana
- Calea zacatechichi
- Silene capensis
- valerian: valerian (the chemical with the same name)
- various plants like chacruna, jurema, vilca, and yopo – 5-MeO-DMT
- Morning glory and Hawaiian Baby Woodrose – lysergic acid amide (LSA, ergine)
- Ayahuasca (for DMT)
- Tabernanthe iboga ("Iboga")—ibogaine
- Areca catechu (see: betel and paan)—arecoline
- Rauvolfia serpentina: rauwolscine
- yohimbe (Pausinystalia johimbe): yohimbine and corynanthine
- many others
Fungi:
- psilocybin mushrooms: psilocybin and psilocin
- various Amanita mushrooms: muscimol
- Amanita muscaria: ibotenic acid and muscimol
- Claviceps purpurea and other Clavicipitaceae: ergotamine (not psychoactive itself but used in synthesis of LSD)
Psychoactive animals:
- hallucinogenic fish
- psychoactive toads: bufotenin, Bufo alvarius (Colorado River toad or Sonoran Desert toad) also contains 5-MeO-DMT
See also
- Alcohol licensing laws of the United Kingdom
- Ban on caffeinated alcoholic drinks in the United States
- Cigarette packets in Australia
- Counterfeit drug
- Demand reduction
- Designer drug
- Drug discovery
- Drug policy
- Drug checking
- Drug education
- Drug policy reform
- Prohibition of drugs
- Effective dose
- Effects of cannabis
- Flavored tobacco
- Gateway drug theory
- Harm reduction
- Illegal drug trade
- LD50
- Legalization of non-medical cannabis in the United States
- Over the counter drug
- Pharmacology
- Polysubstance use and abuse
- Prevalence of tobacco consumption
- Project MKUltra
- Psychedelic experience
- Psychopharmacology
- Psychotomimetism
- Purple drank
- Recreational use of dextromethorphan
- Recreational use of ketamine
- Regulation of therapeutic goods
- Tobacco marketing targeting African Americans
- Tobacco packaging warning messages
- Toxicology
- Usage of electronic cigarettes
Drug-related literature
- Licit and Illicit Drugs
- Marihuana: The First Twelve Thousand Years
- Methland
- Smoke and Mirrors: The War on Drugs and the Politics of Failure
- The Doors of Perception
- The Rhetoric of Drugs
- This Is Your Country On Drugs
References
- Crocq, Marc-Antoine (December 2007). Thibaut, Florence (ed.). "Historical and cultural aspects of man's relationship with addictive drugs". Dialogues in Clinical Neuroscience. Laboratoires Servier. 9 (4): 355–361. doi:10.31887/DCNS.2007.9.4/macrocq. ISSN 1958-5969. OCLC 62869913. PMC 3202501. PMID 18286796. S2CID 12682928.
- Lüscher, C; Ungless, MA (November 2006). Bosurgi, R (ed.). "The Mechanistic Classification of Addictive Drugs". PLOS Medicine. Public Library of Science. 3 (11): e437. doi:10.1371/journal.pmed.0030437. ISSN 1549-1676. LCCN 2004212194. PMC 1635740. PMID 17105338. S2CID 12300815.
- Williams S (24 October 2015). "Specialty Drug Classes That Are Costing Consumers an Arm and a Leg". The Motley Fool.
- Earnshaw, VA (December 2020). "Stigma and substance use disorders: A clinical, research, and advocacy agenda". American Psychologist. American Psychological Association. 75 (9): 1300–1311. doi:10.1037/amp0000744. ISSN 1935-990X. PMC 8168446. PMID 33382299. S2CID 229930928.
- Global Overview of Drug Demand and Supply (PDF). World Drug Report 2017. United Nations. 2017. p. 13. ISBN 978-92-1-148291-1. Retrieved 9 June 2018.
- Staelens S (10 March 2015). "The Bhang Lassi Is How Hindus Drink Themselves High for Shiva". Vice.com. Retrieved 10 August 2017.
- "Drugs, Brains, and Behavior: The Science of Addiction – Drug Misuse and Addiction". www.drugabuse.gov. North Bethesda, Maryland: National Institute on Drug Abuse. 13 July 2020. Retrieved 23 December 2021.
- Plant, MA (September 1980). Marsden, J (ed.). "Drugtaking and prevention: the implications of research for social policy". Addiction. Wiley-Blackwell on behalf of the Society for the Study of Addiction. 75 (3): 245–54. doi:10.1111/j.1360-0443.1980.tb01378.x. ISSN 1360-0443. LCCN 93645978. OCLC 27367194. PMID 6938224. S2CID 32438214.
- White T (2012). Working with Drug and Alcohol Users. London: Jessica Kingsley Publishers. p. 77. ISBN 9780857006189.
- "3.1 Reasons why people use drugs". Australian Department of Health. Archived from the original on 6 November 2021. Retrieved 30 May 2020.
- Sullivan RJ, Hagen EH, Hammerstein P (June 2008). Barrett S (ed.). "Revealing the paradox of drug reward in human evolution" (PDF). Proceedings. Biological Sciences. Royal Society. 275 (1640): 1231–41. doi:10.1098/rspb.2007.1673. ISSN 1471-2954. LCCN 92656221. OCLC 1764614. PMC 2367444. PMID 18353749. S2CID 1102991. Archived (PDF) from the original on 28 December 2021. Retrieved 28 December 2021.
- Sullivan RJ, Hagen EH, Hammerstein P (April 2002). Marsden J (ed.). "Psychotropic substance-seeking: evolutionary pathology or adaptation?". Addiction. 97 (4): 389–400. doi:10.1046/j.1360-0443.2002.00024.x. ISSN 1360-0443. LCCN 93645978. OCLC 27367194. PMID 11964056. S2CID 16713730.
- Nutt D, King LA, Saulsbury W, Blakemore C (March 2007). Horton R (ed.). "Development of a rational scale to assess the harm of drugs of potential misuse". The Lancet. Elsevier. 369 (9566): 1047–53. doi:10.1016/s0140-6736(07)60464-4. ISSN 1474-547X. LCCN sf82002015. OCLC 01755507. PMID 17382831. S2CID 5903121.
- Williams, AR (June 2020). "Cannabis as a Gateway Drug for Opioid Use Disorder". Journal of Law, Medicine & Ethics. Cambridge University Press on behalf of the American Society of Law, Medicine & Ethics. 48 (2: Opioid Controversies: The Crisis – Causes and Solutions): 268–274. doi:10.1177/1073110520935338. ISSN 1748-720X. PMC 7359408. PMID 32631185. S2CID 220385267.
- Ren, M; Lotfipour, S (September 2019). "Nicotine Gateway Effects on Adolescent Substance Use". Western Journal of Emergency Medicine. eScholarship. 20 (5): 696–709. doi:10.5811/westjem.2019.7.41661. ISSN 1936-9018. PMC 6754186. PMID 31539325. S2CID 201978284.
- Balon, R (October 2018). "Illegal or Legal, Marijuana Remains a Gateway Drug". Focus: The Journal of Lifelong Learning in Psychiatry. American Psychiatric Association. 16 (4): 2s–3s. doi:10.1176/appi.focus.164S01. ISSN 1541-4108. PMC 6493246. PMID 31975938. S2CID 169336920.
- Barry, AE; King, J; Sears, C; Harville, C; Bondoc, I; Joseph, K (January 2016). "Prioritizing Alcohol Prevention: Establishing Alcohol as the Gateway Drug and Linking Age of First Drink with Illicit Drug Use". Journal of School Health. Wiley-Blackwell on behalf of the American School Health Association. 86 (1): 31–38. doi:10.1111/josh.12351. ISSN 1746-1561. PMID 26645418. S2CID 8906331.
- Attia, J; Campbell, E; Dray, J; Bowman, J; Freund, M; Hodder, RK; Lecathelinais, C; Oldmeadow, C; Wiggers, J; Wolfenden, L (August 2017). "Effectiveness of a pragmatic school-based universal resilience intervention in reducing tobacco, alcohol, and illicit substance use in a population of adolescents: Cluster-randomised controlled trial" (PDF). BMJ Open. BMJ Group. 7 (8): e016060. doi:10.1136/bmjopen-2017-016060. ISSN 2044-6055. PMC 5629645. PMID 28821523. S2CID 1475517. Archived (PDF) from the original on 30 April 2019. Retrieved 1 October 2021.
- Parker, EM; Bradshaw, CP (October 2015). "Teen Dating Violence Victimization and Patterns of Substance Use Among High School Students". Journal of Adolescent Health. Elsevier on behalf of the Society for Adolescent Health and Medicine. 57 (4): 441–447. doi:10.1016/j.jadohealth.2015.06.013. ISSN 1054-139X. PMID 26271161. S2CID 40481423.
- Chen, CM; Moss, HB; Yi, HY (March 2014). "Early adolescent patterns of alcohol, cigarettes, and marijuana polysubstance use and young adult substance use outcomes in a nationally representative sample". Drug and Alcohol Dependence. Elsevier. 136: 51–62. doi:10.1016/j.drugalcdep.2013.12.011. ISSN 0376-8716. PMID 24434016. S2CID 13003820.
- Chiva-Blanch, G; Badimon, L (January 2020). "Benefits and Risks of Moderate Alcohol Consumption on Cardiovascular Disease: Current Findings and Controversies" (PDF). Nutrients. MDPI. 12 (1: Alcoholic Beverages and Human Health): 108. doi:10.3390/nu12010108. ISSN 2072-6643. PMC 7020057. PMID 31906033. S2CID 210042186. Archived (PDF) from the original on 11 October 2021. Retrieved 11 October 2021.
- Ferrières, J (January 2004). Otto, C (ed.). "The French paradox: lessons for other countries" (PDF). Heart. BMJ Group. 90 (1): 107–111. doi:10.1136/heart.90.1.107. ISSN 1468-201X. PMC 1768013. PMID 14676260. S2CID 6738125. Archived (PDF) from the original on 10 August 2021. Retrieved 21 November 2021.
- "The Nutrition Source: "Drinks to Consume in Moderation – Alcohol: Balancing Risks and Benefits"". www.hsph.harvard.edu. Boston: Department of Nutrition at the Harvard T.H. Chan School of Public Health. 2021. Archived from the original on 11 October 2021. Retrieved 11 October 2021.
- Stampfer MJ, Kang JH, Chen J, Cherry R, Grodstein F (January 2005). "Effects of moderate alcohol consumption on cognitive function in women". The New England Journal of Medicine. Massachusetts Medical Society. 352 (3): 245–253. doi:10.1056/NEJMoa041152. PMID 15659724. S2CID 42052640.
- Nutt D (7 March 2011). "There is no such thing as a safe level of alcohol consumption". The Guardian.
- Nutt DJ, King LA, Phillips LD (November 2010). "Drug harms in the UK: a multicriteria decision analysis". Lancet. London, England. 376 (9752): 1558–65. doi:10.1016/S0140-6736(10)61462-6. PMID 21036393. S2CID 5667719.
- Thomas Nordegren (2002). The A-Z Encyclopedia of Alcohol and Drug Abuse. Parkland, Fla.: Brown Walker Press. p. 327. ISBN 1-58112-404-X.
- Thomas Nordegren (2002). The A-Z Encyclopedia of Alcohol and Drug Abuse. Parkland, Fla.: Brown Walker Press. p. 597. ISBN 1-58112-404-X.
- Blakemore, Colin; Saulsbury, William; King, Leslie A.; Nutt, David (24 March 2007). "Development of a rational scale to assess the harm of drugs of potential misuse". The Lancet. 369 (9566): 1047–1053. doi:10.1016/S0140-6736(07)60464-4. ISSN 0140-6736. PMID 17382831. S2CID 5903121.
- Fish, Jefferson M. (2006). Drugs and Society: U.S. Public Policy. Rowman & Littlefield. ISBN 9780742542457.
- Faupel CE, Horowitz AM, Weaver GS (2004). The Sociology of American Drug Use. Boston: McGraw-Hill Higher Education. p. 366. ISBN 978-0-07-240683-2.
- "Failed states and failed policies, How to stop the drug wars". The Economist. 5 March 2009. Retrieved 10 March 2009.
- Moyer VA (May 2014). "Primary care behavioral interventions to reduce illicit drug and nonmedical pharmaceutical use in children and adolescents: U.S. Preventive Services Task Force recommendation statement". Annals of Internal Medicine. 160 (9): 634–9. doi:10.7326/m14-0334. PMID 24615535.
- Lord S, Marsch L (December 2011). "Emerging trends and innovations in the identification and management of drug use among adolescents and young adults". Adolescent Medicine. 22 (3): 649–69, xiv. PMC 4119795. PMID 22423469.
- Martens MP, Page JC, Mowry ES, Damann KM, Taylor KK, Cimini MD (2006). "Differences between actual and perceived student norms: an examination of alcohol use, drug use, and sexual behavior". Journal of American College Health. 54 (5): 295–300. doi:10.3200/JACH.54.5.295-300. PMID 16539222. S2CID 38595391.
- WHO Report on the Global Tobacco Epidemic 2008: the MPOWER Package (PDF). Geneva: World Health Organization. 2008. ISBN 9789241596282.
- Global status report on alcohol (PDF) (2nd ed.). Geneva: World Health Organization, Dept. of Mental Health and Substance Abuse. 2004. ISBN 9241562722.
- "National Drug Strategy Household Survey 2016: detailed findings". Australian Institute of Health and Welfare. The Australian Institute of Health and Welfare. 28 September 2017.
- Bostwick JM (February 2012). "Blurred boundaries: the therapeutics and politics of medical marijuana". Mayo Clinic Proceedings. Elsevier on behalf of the Mayo Clinic. 87 (2): 172–86. doi:10.1016/j.mayocp.2011.10.003. LCCN sc78001722. PMC 3538401. PMID 22305029. S2CID 8654553. Archived from the original on 14 November 2020. Retrieved 20 August 2021.
- Aikins RD (2 January 2015). "From recreational to functional drug use: the evolution of drugs in American higher education, 1960-2014". History of Education. 44 (1): 25–43. doi:10.1080/0046760X.2014.979251. PMC 4972325. PMID 27499559.
- Farber D (2004). The Sixties Chronicle. Legacy Publishing. p. 432. ISBN 978-1412710091.
- Robison J (2 July 2002). "Decades of Drug Use: Data From the '60s and '70s". Gallup.com. Retrieved 13 November 2013.
- "Marijuana: History of Marijuana Use". The Columbia Electronic Encyclopedia (6th ed.). Columbia University Press. 2012. OCLC 746941797 – via infoplease.com.
- Di Forti M (June 2020). Maj M (ed.). "To legalize or not to legalize cannabis, that is the question!". World Psychiatry. Wiley-Blackwell on behalf of the World Psychiatric Association. 19 (2): 188–189. doi:10.1002/wps.20737. PMC 7214953. PMID 32394550. S2CID 218598941.
- Bahji A, Stephenson C (August 2019). "International Perspectives on the Implications of Cannabis Legalization: A Systematic Review & Thematic Analysis". International Journal of Environmental Research and Public Health. MDPI. 16 (17): 3095. doi:10.3390/ijerph16173095. PMC 6747067. PMID 31454942. S2CID 201658917.
- Pacula RL, Smart R (May 2017). Cannon T, Widiger T (eds.). "Medical Marijuana and Marijuana Legalization". Annual Review of Clinical Psychology. Annual Reviews. 13: 397–419. doi:10.1146/annurev-clinpsy-032816-045128. LCCN 2004212108. PMC 6358421. PMID 28482686. S2CID 3836912.
- Hunt, Geoffrey; Milhet, Maitena; Bergeron, Henri, eds. (2016). "Part II - Consumption: Cultures of Drug Use". Drugs and Culture: Knowledge, Consumption, and Policy. London and New York: Routledge. pp. 113–194. ISBN 9781138274426. LCCN 2010048568.
- Haenfler, Ross (2015). "Straight Edge". In Parmar, Priya; Nocella II, Anthony J.; Robertson, Scott; Diaz, Martha (eds.). Rebel Music: Resistance through Hip Hop and Punk. Charlotte, North Carolina: Information Age Publishing. pp. 137–138. ISBN 978-1-62396-910-3.
- Weir E (June 2000). "Raves: a review of the culture, the drugs and the prevention of harm" (PDF). CMAJ. Canadian Medical Association. 162 (13): 1843–8. eISSN 1488-2329. LCCN 87039047. PMC 1231377. PMID 10906922. S2CID 10853457. Archived (PDF) from the original on 28 June 2019. Retrieved 17 August 2021.
- Smith KM, Larive LL, Romanelli F (June 2002). "Club drugs: methylenedioxymethamphetamine, flunitrazepam, ketamine hydrochloride, and gamma-hydroxybutyrate". American Journal of Health-System Pharmacy. American Society of Health-System Pharmacists. 59 (11): 1067–76. doi:10.1093/ajhp/59.11.1067. eISSN 1535-2900. OCLC 41233599. PMID 12063892. S2CID 44680086.
- Klein M, Kramer F (February 2004). "Rave drugs: pharmacological considerations" (PDF). AANA Journal. American Association of Nurse Anesthetists. 72 (1): 61–7. PMID 15098519. S2CID 41926572. Archived (PDF) from the original on 17 August 2021. Retrieved 17 August 2021.
- Degenhardt L, Copeland J, Dillon P (2005). "Recent trends in the use of "club drugs": an Australian review". Substance Use & Misuse. Taylor & Francis. 40 (9–10): 1241–56. doi:10.1081/JA-200066777. eISSN 1532-2491. LCCN 2006268261. PMID 16048815. S2CID 25509945.
- Halpern P, Moskovich J, Avrahami B, Bentur Y, Soffer D, Peleg K (April 2011). "Morbidity associated with MDMA (ecstasy) abuse: a survey of emergency department admissions". Human & Experimental Toxicology. SAGE Publications. 30 (4): 259–66. doi:10.1177/0960327110370984. eISSN 1477-0903. LCCN 90031138. PMID 20488845. S2CID 30994214.
- Palamar JJ, Acosta P, Le A, Cleland CM, Nelson LS (November 2019). "Adverse drug-related effects among electronic dance music party attendees". International Journal of Drug Policy. Elsevier. 73: 81–87. doi:10.1016/j.drugpo.2019.07.005. ISSN 1873-4758. PMC 6899195. PMID 31349134. S2CID 198932918.
- Wu LT, Schlenger WE, Galvin DM (September 2006). "Concurrent use of methamphetamine, MDMA, LSD, ketamine, GHB, and flunitrazepam among American youths". Drug and Alcohol Dependence. Elsevier. 84 (1): 102–13. doi:10.1016/j.drugalcdep.2006.01.002. PMC 1609189. PMID 16483730. S2CID 24699584.
- Gonzales, Matt (2 March 2020) [27 November 2017]. "Rap Culture's Evolution from Glorifying to Decrying Drug Use". Orlando, Florida: DrugRehab.com. Archived from the original on 16 January 2021. Retrieved 10 January 2022.
- "Can Hip-Hop Separate Itself From The Drug Culture It Helped Build?". CULTR. 18 December 2019. Archived from the original on 5 December 2020. Retrieved 10 January 2022.
- Granovsky, Josh (23 November 2018). "Emo rap needs to end". The Queen's Journal. Kingston, Ontario: Alma Mater Society of Queen's University. Archived from the original on 24 July 2021. Retrieved 7 August 2022.
- Smiley, Calvin J. (2017). "Addict Rap?: The Shift from Drug Distributor to Drug Consumer in Hip Hop" (PDF). Journal of Hip Hop Studies. Richmond, Virginia: VCU Scholars Compass (Virginia Commonwealth University). 4 (1): 1–24. doi:10.34718/ZBWC-RN03. ISSN 2331-5563. Archived from the original on 6 July 2021. Retrieved 10 January 2022.
- "Commonly Used Drugs Charts". National Institute on Drug Abuse. 20 August 2020. Retrieved 8 October 2020.
- The International Agency for Research on Cancer (IARC). "Agents Classified by the IARC Monographs" (PDF). IARC Monographs on the Identification of Carcinogenic Hazards to Humans. Vol. 1–120. World Health Organization (WHO). Archived from the original (PDF) on 28 March 2018.
- Trevisan LA, Boutros N, Petrakis IL, Krystal JH (1998). "Complications of alcohol withdrawal: pathophysiological insights" (PDF). Alcohol Health and Research World. 22 (1): 61–6. PMC 6761825. PMID 15706735.
- Jenkins JP. "Methamphetamine (drug)". Britannica Online Encyclopedia. Retrieved 29 January 2012.
- Cruickshank CC, Dyer KR (July 2009). "A review of the clinical pharmacology of methamphetamine". Addiction. 104 (7): 1085–99. doi:10.1111/j.1360-0443.2009.02564.x. PMID 19426289. S2CID 37079117.
- Malenka RC, Nestler EJ, Hyman SE (2009). "15". In Sydor A, Brown RY (eds.). Molecular Neuropharmacology: A Foundation for Clinical Neuroscience (2nd ed.). New York: McGraw-Hill Medical. p. 370. ISBN 978-0-07-148127-4.
Unlike cocaine and amphetamine, methamphetamine is directly toxic to midbrain dopamine neurons.
- Nestler EJ (2009). Molecular neuropharmacology : a foundation for clinical neuroscience. Hyman, Steven E., Malenka, Robert C. (2nd ed.). New York: McGraw-Hill Medical. p. 375. ISBN 9780071641197. OCLC 273018757.
- Scheidweiler KB, Plessinger MA, Shojaie J, Wood RW, Kwong TC (December 2003). "Pharmacokinetics and pharmacodynamics of methylecgonidine, a crack cocaine pyrolyzate". Journal of Pharmacology and Experimental Therapeutics. 307 (3): 1179–87. doi:10.1124/jpet.103.055434. PMID 14561847. S2CID 15619796.
- Yang Y, Ke Q, Cai J, Xiao YF, Morgan JP (January 2001). "Evidence for cocaine and methylecgonidine stimulation of M(2) muscarinic receptors in cultured human embryonic lung cells". British Journal of Pharmacology. 132 (2): 451–60. doi:10.1038/sj.bjp.0703819. PMC 1572570. PMID 11159694.
- Fandiño AS, Toennes SW, Kauert GF (December 2002). "Studies on hydrolytic and oxidative metabolic pathways of anhydroecgonine methyl ester (methylecgonidine) using microsomal preparations from rat organs". Chemical Research in Toxicology. 15 (12): 1543–8. doi:10.1021/tx0255828. PMID 12482236.
- Rahman MA, Hann N, Wilson A, Worrall-Carter L (2014). "Electronic cigarettes: patterns of use, health effects, use in smoking cessation and regulatory issues". Tobacco Induced Diseases. 12 (1): 21. doi:10.1186/1617-9625-12-21. PMC 4350653. PMID 25745382.
- Burstyn I (January 2014). "Peering through the mist: systematic review of what the chemistry of contaminants in electronic cigarettes tells us about health risks". BMC Public Health. 14: 18. doi:10.1186/1471-2458-14-18. PMC 3937158. PMID 24406205.
- Grana R, Benowitz N, Glantz SA (May 2014). "E-cigarettes: a scientific review". Circulation. 129 (19): 1972–86. doi:10.1161/circulationaha.114.007667. PMC 4018182. PMID 24821826.
- Holbrook BD (June 2016). "The effects of nicotine on human fetal development". Birth Defects Research. Part C, Embryo Today. 108 (2): 181–92. doi:10.1002/bdrc.21128. PMID 27297020.
- Siqueira LM (January 2017). "Nicotine and Tobacco as Substances of Abuse in Children and Adolescents". Pediatrics. 139 (1): e20163436. doi:10.1542/peds.2016-3436. PMID 27994114.
- Jenssen BP, Boykan R (February 2019). "Electronic Cigarettes and Youth in the United States: A Call to Action (at the Local, National and Global Levels)". Children. 6 (2): 30. doi:10.3390/children6020030. PMC 6406299. PMID 30791645.
- Breitbarth AK, Morgan J, Jones AL (November 2018). "E-cigarettes-An unintended illicit drug delivery system". Drug and Alcohol Dependence. 192: 98–111. doi:10.1016/j.drugalcdep.2018.07.031. PMID 30245461.
- Hofmann A. "LSD My Problem Child". Archived from the original on 11 January 2010. Retrieved 19 April 2010.
- Brecher EM, et al. (The Editors of Consumer Reports Magazine) (1972). "Chapter 50. How LSD was popularized, 1962-1969". The Consumers Union Report on Licit and Illicit Drugs.
- United States Congress (24 October 1968). "Staggers-Dodd Bill, Public Law 90-639" (PDF). Retrieved 8 September 2009.
- Hofmann A, Heim R, Tscherter H (1963). ""Phytochimie – présence de la psilocybine dans une espèce européenne d'agaric, le Psilocybe semilanceata Fr."" [Phytochemistry – presence of psilocybin in a European agaric species, Psilocybe semilanceata]. Comptes rendus hebdomadaires des séances de l'Académie des sciences (in French). 257 (1): 10–12.
- Wonnacott S (February 1997). "Presynaptic nicotinic ACh receptors". Trends in Neurosciences. 20 (2): 92–8. doi:10.1016/S0166-2236(96)10073-4. PMID 9023878. S2CID 42215860.
- Power, Mike (5 June 2020). "I Sell DMT Vape Pens So People Can 'Break Through' at Their Own Speed". www.vice.com. Retrieved 4 January 2022.
{{cite web}}: CS1 maint: url-status (link) - "Erowid DMT (Dimethyltryptamine) Vault". www.erowid.org. Retrieved 4 January 2022.
- Smith L (22 May 2018). "The drug plague destroying families across South Africa". Zululand Observer. Retrieved 14 July 2020.
- "Quaaludes (methaqualone) Uses, Effects & History of Abuse". Drugs.com. Retrieved 14 July 2020.
- "Ativan 1 mg Sublingual Tablets". Malahyde Information Systems. 3 May 1985. Archived from the original on 4 February 2004. Retrieved 8 July 2016.
- Ruiz, María Esperanza; Scioli Montoto, Sebastián (2018), Talevi, Alan; Quiroga, Pablo A. M. (eds.), "Routes of Drug Administration", ADME Processes in Pharmaceutical Sciences, Cham: Springer International Publishing, pp. 97–133, doi:10.1007/978-3-319-99593-9_6, ISBN 978-3-319-99592-2, retrieved 27 March 2022
- Verma, P.; Thakur, A.S.; Deshmuhk, K.; Jha, A.K.; Verma, S. "Routes of Drug Administration" (PDF). International Journal of Pharmaceutical Studies and Research.
- Latkin, Carl A; Knowlton, Amy R; Sherman, Susan (1 September 2001). "Routes of drug administration, differential affiliation, and lifestyle stability among cocaine and opiate users: Implications to HIV prevention". Journal of Substance Abuse. SUBSTANCE ABUSE AND HIV. 13 (1): 89–102. doi:10.1016/S0899-3289(01)00070-0. ISSN 0899-3289. PMID 11547627.
- Gossop, Michael; Marsden, John; Stewart, Duncan; Treacy, Samantha (August 2000). "Routes of drug administration and multiple drug misuse: regional variations among clients seeking treatment at programmes throughout England". Addiction. 95 (8): 1197–1206. doi:10.1046/j.1360-0443.2000.95811976.x. ISSN 0965-2140. PMID 11092067.
- "Depressant". MSDS Glossary. Environmental Health and Safety, University of Texas at Austin. 30 August 2007. Archived from the original on 17 January 2009. Retrieved 1 January 2009.
- Murrie B, Lappin J, Large M, Sara G (April 2020). "Transition of Substance-Induced, Brief, and Atypical Psychoses to Schizophrenia: A Systematic Review and Meta-analysis". Schizophrenia Bulletin. 46 (3): 505–516. doi:10.1093/schbul/sbz102. PMC 7147575. PMID 31618428.
- "Psychostimulant". Dorlands Medical Dictionary.
- Morgan CJ, Badawy AA (2001). "Alcohol-induced euphoria: exclusion of serotonin". Alcohol and Alcoholism. 36 (1): 22–5. doi:10.1093/alcalc/36.1.22. PMID 11139411.
- Foster S (2002). A field guide to Western Medicinal Plants and Herbs. New York: Houghton Mifflin Company. p. 58. ISBN 978-0395838068.
- Cuthbert AW (2001). "Stimulants". In Blakemore C, Jennett S (eds.). The Oxford companion to The body. Oxford: Oxford University Press. ISBN 978-0-19-852403-8.
- Hayward R (2001). "Euphoria". In Blakemore C, Jennett S (eds.). The Oxford companion to The body. Oxford: Oxford University Press. ISBN 978-0-19-852403-8.
- "Ecstasy". The World Encyclopedia. New York, N.Y.: Oxford University Press. 2001. doi:10.1093/acref/9780199546091.001.0001. ISBN 978-0-19-954609-1.
- "Opium". The World Encyclopedia. New York, N.Y.: Oxford University Press. 2001. doi:10.1093/acref/9780199546091.001.0001. ISBN 978-0-19-954609-1.
- Quax, Marcel L. J.; Van Der Steenhoven, Timothy J.; Bronkhorst, Martinus W. G. A.; Emmink, Benjamin L. (July 2020). "Frostbite injury: An unknown risk when using nitrous oxide as a party drug". Acta Chirurgica Belgica. Taylor & Francis on behalf of the Royal Belgian Society for Surgery. 120 (1–4): 140–143. doi:10.1080/00015458.2020.1782160. ISSN 0001-5458. PMID 32543291. S2CID 219702849.
- Edwards RW, Oetting ER (1995). "Inhalant use in the United States". In Kozel N, Sloboda Z, De La Rosa M (eds.). Epidemiology of Inhalant Abuse: An International Perspective. Proceedings of a meeting. July 21-22, 1993 (PDF). NIDA Research Monograph. Vol. 148. pp. 8–28. PMID 8999334. Archived from the original (PDF) on 26 September 2006.
- "Inhalants". Greater Dallas Council on Alcohol & Drug Abuse. Archived from the original on 8 April 2009.
Further reading
- Martin, Christopher S.; Chung, Tammy; Langenbucher, James W. (2017). "Part 1: Defining and Characterizing the Nature and Extent of Substance Use Disorders – Historical and Cultural Perspectives on Substance Use and Substance Use Disorders". In Sher, Kenneth J. (ed.). The Oxford Handbook of Substance Use and Substance Use Disorders: Volume 1. Oxford Library of Psychology. Oxford and New York: Oxford University Press. pp. 27–59. doi:10.1093/oxfordhb/9780199381678.013.001. ISBN 9780199381678. LCCN 2016020729.
- Anthony, James; Barondess, David A.; Radovanovic, Mirjana; Lopez-Quintero, Catalina (2017). "Part 1: Psychiatric Comorbidity – Polydrug Use: Research Topics and Issues". In Sher, Kenneth J. (ed.). The Oxford Handbook of Substance Use and Substance Use Disorders: Volume 2. Oxford Library of Psychology. Oxford and New York: Oxford University Press. pp. 27–59. doi:10.1093/oxfordhb/9780199381708.013.006. ISBN 9780199381708. LCCN 2016020729.
- Hernández-Serrano, Olga; Gras, Maria E.; Font-Mayolas, Sílvia; Sullman, Mark J. M. (2016). "Part VI: Dual and Polydrug Abuse – Chapter 83: Types of Polydrug Usage". In Preedy, Victor R. (ed.). Neuropathology of Drug Addictions and Substance Misuse, Volume 3: General Processes and Mechanisms, Prescription Medications, Caffeine and Areca, Polydrug Misuse, Emerging Addictions and Non-Drug Addictions. Cambridge, Massachusetts: Academic Press, imprint of Elsevier. pp. 839–849. doi:10.1016/B978-0-12-800634-4.00083-4. ISBN 978-0-12-800634-4.
External links
- "The Science of Drug Use: A Resource for the Justice Sector". www.drugabuse.gov. North Bethesda, Maryland: National Institute on Drug Abuse. 26 May 2020. Retrieved 23 December 2021.
- School-Based Drug Abuse Prevention: Promising and Successful Programs (PDF). www.publicsafety.gc.ca. Ottawa, Ontario: Public Safety Canada. 31 January 2018. ISBN 978-1-100-12181-9. Archived (PDF) from the original on 19 May 2021. Retrieved 23 December 2021.
- Sacco LN, Finklea K (3 May 2016). "Synthetic Drugs: Overview and Issues for Congress" (PDF). Washington, D.C.: Congressional Research Service. Archived (PDF) from the original on 8 December 2021. Retrieved 23 December 2021.